A general description of the competitive transplant setting, including secondary transplants (discussed further below) can be found in Figure 1. A representative analysis for pre-transplant bone marrow HSCs can be found in Figure 2. More detailed information on the exclusion of doublets and dead cells can be found elsewhere9.
Figures 3 and 4 provide examples of flow cytometry analysis templates for peripheral blood and bone marrow, respectively. It is normal to detect some host T lymphocytes (up to 20% of all T cells; Figure 3B), as T cells are more radio-resistant. Competitor-derived cells should be present in all three lineages. The detection limit depends a lot on the number of total cells acquired for analysis, but in our experience a total of 20 thousand cells within the single leukocyte gate is usually sufficient. Using an arbitrary threshold of 1% or 0.5%, if donor cells represent a lower proportion than the cutoff in any given lineage (B lymphoid, T lymphoid, or myeloid as shown in Figure 3), the mouse is not considered positive for multilineage reconstitution. This concept becomes important when the competitive transplants are combined with a limiting dilution assay to quantify donor HSCs as explained in the discussion. It is certainly possible to have, for example, donor-derived T and B lymphocytes but gradual loss of myeloid cells, which would usually suggest only transient reconstitution. Lymphocytes have longer half-lives than myeloid cells (particularly Gr1hi SSChi granulocytes/neutrophils) and can persist even in the absence of bone marrow HSCs10.
Figure 5 depicts representative results for peripheral blood chimerism under different situations. When donor HSCs are functionally equivalent to competitor cells, the proportions of donor (CD45.2+) and competitor (CD45.1+) -derived cells are equivalent (Figure 5A). The residual host cells (CD45.1+ CD45.2+) in Figure 5A and 5B are almost exclusively T lymphocytes as they are more radio-resistant. When donor cells present a much lower proportion of peripheral blood leukocytes (Figure 5B), some aspects of HSC function are likely defective and further studies are needed as described in the discussion. The presence of competitor cells confirms that the assay worked well but donor bone marrow was simply less effective. This is in contrast to the result presented in Figure 5C, where both donor and competitor cells are present in low numbers and host cells represent the majority of peripheral blood cells. In this case the transplant was unsuccessful and it is not possible to draw any conclusions as to the relative functionality of donor versus competitor cells. Different solutions are discussed further below.
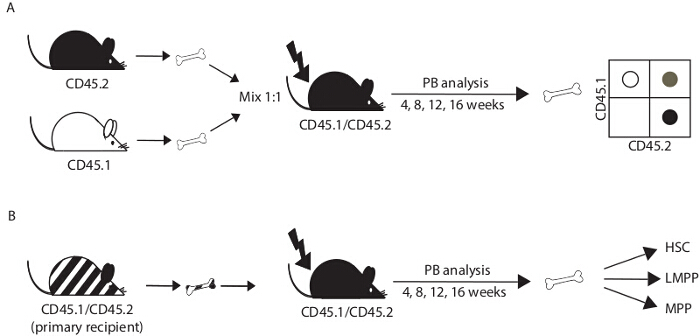
Figure 1. Experimental design. (A) For a competitive transplant, bone marrow cells from donor mice (CD45.2+; C57Bl6 background; control and test) and congenic competitor mice (CD45.1+; B6.SJL) are mixed in a 1:1 ratio and injected into the tail vein of irradiated recipient mice (CD45.1+ CD45.2+; F1 progeny of C57Bl6 x B6.SJL breeding pairs). The efficacy of bone marrow reconstitution is determined in peripheral blood (PB) at 4, 8, 12 and 16 weeks post-transplant and in the bone marrow at 16 weeks after transplant or later. (B) To further evaluate the self-renewal of transplanted cells, bone marrow cells recovered from transplant recipients after 16 weeks can be transferred into irradiated secondary recipient mice. HSC, hematopoietic stem cell; MPP, multipotent progenitor cell; LMPP, lymphoid-primed MPP. Please click here to view a larger version of this figure.
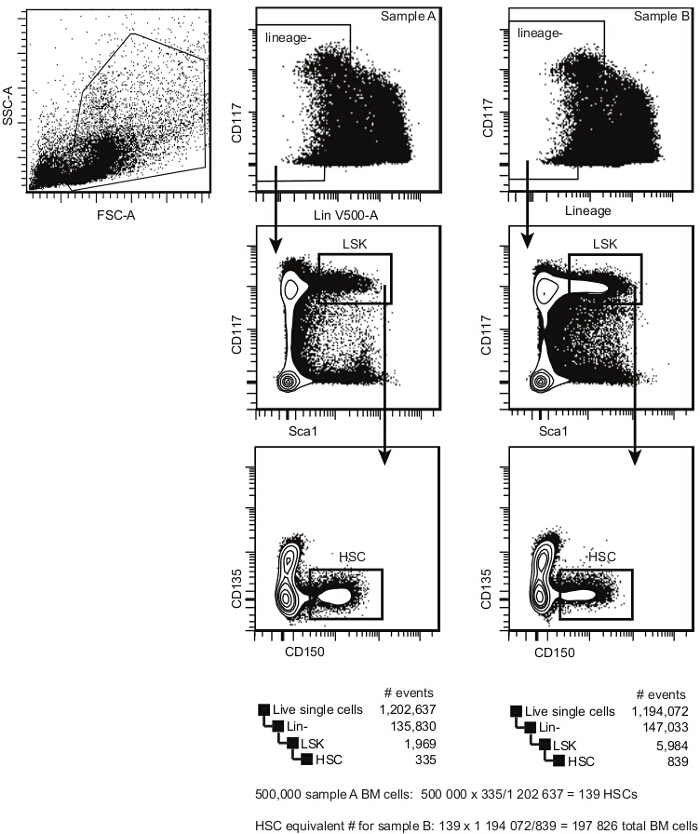
Figure 2. Pre-transplant bone marrow HSC analysis template. Within single cells, select HSPCs according to cKit (CD117) and Lineage expression. Within the Lindim/- cell population, select the cKitbright Sca1+ population (LSK). Within LSKs, select CD150+ CD135– HSCs. This population contains both long-term and short-term repopulating HSCs (the frequency of a repopulating cell within this population is between 1/3 and 1/5). The estimated frequency of bone marrow HSCs is calculated by dividing the number of events in the HSC gate by the number of events in the single cell gate. Please click here to view a larger version of this figure.
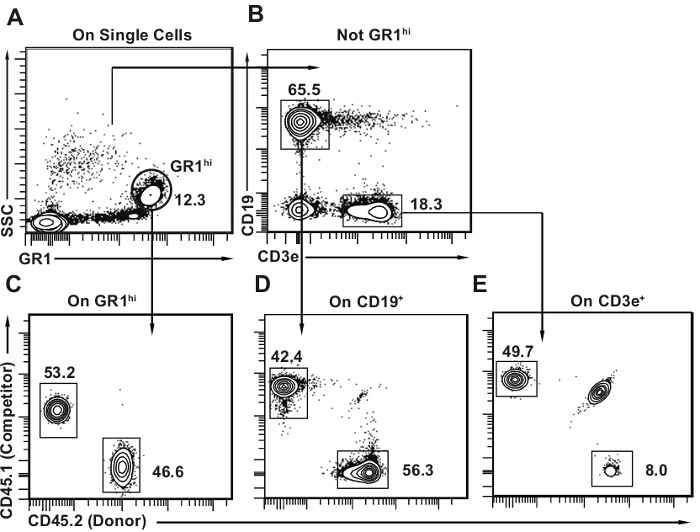
Figure 3. Post-transplant peripheral blood analysis template. (A) Within single cells, select first GR1bright SSChi granulocytes. (B) Then select CD19+ CD3e– B lymphocytes and CD3e+ CD19– T lymphocytes. Mouse peripheral blood contains a large proportion of lymphocytes, with B lymphocytes being the major cell type (approximately 50% all peripheral blood cells). C-E) Draw 2D flow cytometry plots for each subset with CD45.2 on one axis and CD45.1 on the other. Identify donor (CD45.2+), host (CD45.1+ CD45.2+) and competitor cells (CD45.1+) for each lineage as shown. It is normal to have some remaining host cells, particularly in the T lymphocyte population as seen in panel E. Please click here to view a larger version of this figure.
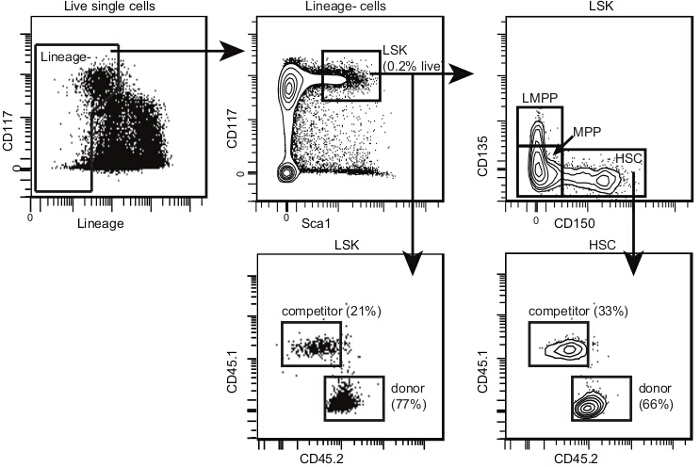
Figure 4. Post-transplant bone marrow HSC analysis template. Within single cells, select HSPCs and LSKs as shown for Figure 2. Within LSKs, select CD150+ CD135- HSCs, CD150- CD135- multipotent progenitors (or MPPs) and CD150- CD135+ lymphoid-primed MPPs (or LMPPs). The proportion of LMPPs is lower after transplant than in non-irradiated mice. Draw 2D flow cytometry plots for each subset with CD45.2 on one axis and CD45.1 on the other. Identify donor, host and competitor cells for each subpopulation as shown. If the irradiation and transplant are successful, there should be very few remaining host HSPCs. Please click here to view a larger version of this figure.
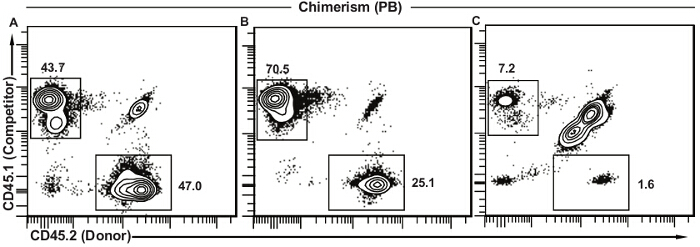
Figure 5. Representative results for peripheral blood chimerism. (A) Successful transplant where donor HSCs are functionally equivalent to the competitor cells. The vast majority of remaining host cells (CD45.1+ CD45.2+) is usually T lymphocytes. (B) Successful transplant where donor HSCs show decreased function as compared to competitor cells. This decreased contribution can be due to several different factors and further analysis will be needed (see discussion). (C) Unsuccessful transplant with low frequencies of both competitor and donor cells and a large proportion of remaining host cells. This type of result suggests a lower than expected dose of irradiation, unsuccessful injection (decreased cell viability, decreased volume of injection, injection outside of the tail vein), or a combination of these. Please click here to view a larger version of this figure.
