Left Anterior Descending Coronary Artery Ligation for Ischemia-Reperfusion Research: Model Improvement via Technical Modifications and Quality Control
Summary
Herein, we present a protocol focusing on the quality control of the left anterior descending coronary artery ligation by technically modifying the traditional procedure in rats for acute myocardial ischemia-reperfusion research.
Abstract
Coronary heart disease is the leading cause of death globally. Complete cessation of blood flow in coronary arteries causes ST-segment elevation myocardial infarction (STEMI), resulting in cardiogenic shock and fatal arrhythmia, which are associated with high mortality. Primary coronary intervention (PCI) for recanalizing the coronary artery significantly improves the outcomes of STEMI, but advancements made in shortening the door-to-balloon time have failed to reduce in-hospital mortality, suggesting that additional therapeutic strategies are required. Left anterior descending coronary artery (LAD) ligation in rats is an animal model for acute myocardial IR research that is comparable to the clinical scenario in which rapid coronary recanalization through PCI is used for STEMI; however, PCI-induced STEMI is a technically challenging and complicated operation associated with high mortality and great variation in infarction size. We identified the ideal position for LAD ligation, created a gadget to control a snare loop, and supported a modified surgical maneuver, thereby reducing tissue damage, to establish a reliable and reproducible acute myocardial ischemia-reperfusion (IR) research protocol for rats. This is a non-survival surgery. We also propose a method for validating the quality of study results, which is a critical step for determining the accuracy of subsequent biochemical analyses.
Introduction
Ischemic heart disease is a leading cause of death worldwide1,2. In addition to the control of modifiable risk factors for preventing the development of coronary heart disease, therapeutic strategies are crucially required for acute coronary syndrome3,4. Cardiogenic shock and fatal arrhythmia in acute ST-segment elevation myocardial infarction (STEMI) have been found to increase the likelihood of in-hospital mortality5,6,7,8. Primary percutaneous coronary intervention (PCI) is the preferred treatment for STEMI9,10,11; however, the therapeutic effects have a ceiling when the door-to-balloon time is <90 min12,13. Additional strategies are required for further improving the clinical outcomes of the disease14,15,16,17,18,19.
An acute myocardial ischemia- reperfusion (IR) experiment involving left anterior descending artery (LAD) ligation in rats is one of the animal models comparable to the clinical scenario wherein short door-to-balloon times are required for patients with STEMI to rescue the heart from ischemic damage. However, surgery-induced STEMI in small animals is often technically challenging because it is a complex operation associated with high mortality and high variation in infarction size20,21,22,23,24. To overcome the technical challenge, the present study developed a comprehensive and effective animal model in rats (because they are larger than mice) to establish a reliable and reproducible acute myocardial IR research protocol through technical modification. The proposed protocol results in fewer surgical complications, less tissue damage, and less likelihood of mortality during surgery. Additionally, a procedure was used to measure the infarct size and area at risk (AAR) and, thus, verify the quality of the study results. The proposed protocol can be used to investigate the pathophysiological processes of acute myocardial IR stress to develop new therapeutic strategies against the damage.
Protocol
All animal experiments were conducted in accordance with the Guide for the Care and Use of Laboratory Animals, published by the US National Institutes of Health (NIH publication no. 85-23, revised 1996). The study protocol was approved by and in accordance with the guidelines of the Institutional Animal Care and Use Committee at Fu-Jen Catholic University.
1. Preparation before surgery
- Preparation of saline wet cotton balls
- Put on a surgical mask and gloves.
- Pinch off a small portion of sterile cotton and roll it to form a ball. Repeat this procedure.
- Dip the cotton balls in sterile 0.9% saline and squeeze out excess saline.
- Store the cotton balls in a clean box sterilized with 75% ethanol.
- Preparation of holding hooks.
- Put on a surgical mask and gloves.
- Sterilize clips and rubber bands with 75% ethanol.
- Bend the clips into the shape of a hook for the chest wall and tissue.
- Connect the bent clips with one, two, or three rubber bands to ensure the tension from the wound of the surgical window is wide enough for LAD ligation.
- Prepare and store at least five homemade hooks in a clean box sterilized with 75% ethanol.
- Preparation of a ligation loop.
- Place the middle of a 7-0 silk stitch in the 1/2 circle size 3 spring eye of a tapered nonswaged surgical needle.
- Preparation of a snare loop controller
- Cut a 5-mm polyethylene (PE)-10 tube using scissors.
- Heat and soften the tube under flame to smooth both of its edges.
- Preparing the rats
- Select 8-week-old Sprague-Dawley male rats with a minimum weight of 250 g.
- House and maintain the rats under a 12 h light/dark cycle at a controlled temperature (21 °C ± 2 °C) with free access to food, standard mouse pellets, and tap water.
- Anesthetize the rats with pentobarbital (50 mg/kg, administered intraperitoneally).
NOTE: Additional anesthetic (pentobarbital, 30 mg/kg) should be administered after every hour. - Check the rats' reflexes by pinching the tail and hind feet to ensure that the animal is sufficiently anesthetized.
- Open the tissue between two cartridge rings below the glottis using scissors and insert a 3 cm PE-10 tube to act as an endotracheal tube25.
- Connect the endotracheal tube to a ventilator manually.
- Inspect the animal's thoracic movement synchronized with the respiration cycle to ensure the lungs are adequately ventilated.
- Open the neck region and cannulate the jugular vein26.
2. LAD ligation
- Put on a surgical mask and gloves.
- Touch the chest and find the manubrium and sternal angle (the junction of the manubrium and sternum body).
- Identify the left-side rib that connects with the sternal angle (rib A) by touching manually.
- Identify the intercostal space immediately below rib A. Use fine-tip forceps to gently lift the skin close to the intercostal space, and then use a surgical scalpel with a blade to create a 1 cm oblique incision along the skin tension lines from the point approximately 5 mm to the left of the sternal body.
- Use curved forceps to gently separate the skin and muscle layers from the incision. Hook the muscle layers outside the left anterior chest wall downward with bent clips to expose the ribs underneath.
- Identify the rib below rib A (rib B). Cut rib B with a blunt scissor from the middle of the rib cartilage (approximately 2-3 mm from the sternal body). Gently touch and compress the wound with a saline wet cotton ball for several seconds if bleeding occurs.
- Open the thorax carefully from the cut of rib B with four bent clips. Each bent clip should hook the intercostal muscle and ribs to gently spread the chest wall in four directions (namely, upper then left, upper then right, left downward, and right downward) and create a rectangular surgical window.
- Hook gently against the left lung and other adjacent tissues covering the pericardium with another bent clip to prevent accidental tissue damage during the procedure.
- Expose the heart by gently removing the thin pericardium with forceps. Identify the 1st branch of the left main coronary artery (LMCA), which is usually between the pulmonary artery and left auricle. The LMCA and LAD present as a superficial bright red line that runs from the edge of the left auricle toward the apex.
- Use the prepared surgical needle to create an open ligation loop by inserting and passing the silk stitch under the LAD at a location immediately distal to the 1st branch of the LMCA in the direction from the left toward the right side of the LAD to avoid accidentally puncturing the left auricle. With a single suture, the open loop is created. Gently swab the surface of the heart to visualizethe coronary arteries if the LAD is invisible because of fluid or blood covering the surface of the heart.
- Hold one side of the suture and gently separate the needle from the suture using a needle holder.
- Insert the two ends of the silk suture on one side of the open loop into the circle on the other side to form a snare loop.
- Insert the two ends of the silk suture of the snare loop into the prepared snare controller before closing the loop.
- Slide the snare loop controller along the silk suture while gently stretching the silk to close the snare loop. Cease the coronary flow of the LAD to induce temporary myocardial ischemia for 1 h.
- Hold the silk to fix the position of the snare loop controller with Kelly forceps once the loop has been tied securely. Place the other end of the Kelly forceps on the surgical table during LAD ligation.
- Cover the surgical window with saline wet cotton balls during LAD ligation.
- Open the Kelly forceps.
- Release the snare loop controller for reperfusion of the coronary flow for 2 h.
- Resect the heart along the base and vascular borders carefully and avoid grabbing the tissue.
NOTE: Euthanize the rat with CO2 at a flow rate of 40% cage volume/min.
Representative Results
At the end of myocardial ischemia and reperfusion, the quality of LAD ligation should be assessed before further biochemical or molecular analyses.
The sufficiency of LAD occlusion through ligation was determined by injecting 1 mL of 2% Evan's blue dye through the central venous catheter. Then, the myocardium with coronary perfusion was stained blue compared with the non-perfused region, which remained red (Figure 1A). The red region is the AAR of myocardial infarction.
The accuracy of the location for LAD ligation was further evaluated by quantifying the variation in AAR percentage among the study animals. After the heart was sliced horizontally, the AAR percentage was determined by dividing the AAR by the whole myocardial mass (Figure 1B). A low variation in AAR percentage among the study animals indicated accurate location of the LAD ligation.
The myocardial infarct size is the primary result in acute myocardial IR research. To quantify this parameter, the sliced heart sections were incubated in 1% 2,3,5-triphenyltetrazolium chloride (TTC) in normal saline at 37 °C for 30 min and then in 10% formaldehyde for 3 days. The infarct area was white. The infarct size percentage was calculated as the ratio of the infarct area to the AAR (Figure 2).
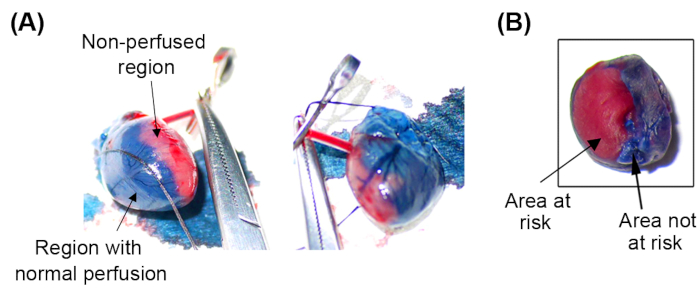
Figure 1: Validation of LAD ligation quality with Evan's blue. (A) The AAR for myocardial infarction was the non-perfused myocardial mass that remained red even after Evan's blue was injected, thereby confirming secure LAD ligation. (B) The AAR percentage was calculated by dividing the AAR (red area) by the whole myocardial mass (red and blue area); a low variation in AAR percentage among the study animals demonstrated accurate location of the LAD ligation. A smaller infarct size was demonstrated in drug-treated groups as compared to non-treated groups. AAR, area at risk; LAD, left anterior descending artery. Please click here to view a larger version of this figure.
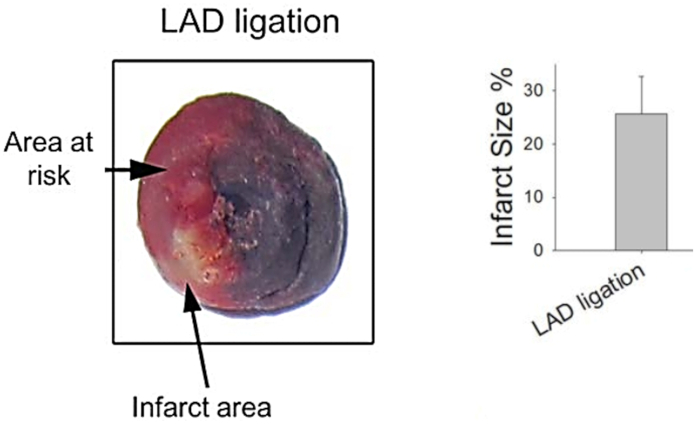
Figure 2: Quantification of myocardial infarct size in TTC treatment. Infarct size was estimated as the ratio of the infarct area (white area) to the AAR (red area) in the LAD ligation group. AAR, area at risk; TTC, triphenyltetrazolium chloride. Please click here to view a larger version of this figure.
Discussion
The proposed protocol has several distinctive features, such as identifying the exact position for LAD ligation, creating a gadget to control a snare loop in a single suture, and supporting a modified surgical maneuver to reduce tissue damage, thus enabling researchers to ligate the LAD accurately, securely, and consistently, as well as control the state of the snare loop instantly for acute myocardial IR research.
The location of LAD ligation influences the area and size of the myocardial infarction. Ligation is generally suggested at a certain distance on the proximal LAD27,28. Overlooking the variance in coronary artery branching patterns may increase the variability in myocardial infarction23,24. In this study, the LAD was ligated immediately distal to the 1st branch of the LMCA, thus preventing accidental ligation of the left circumflex artery or septal artery and leading to consistent infarct size and a lower likelihood of fatal arrhythmia29,30,31.
Secure LAD ligation is essential for LAD occlusion. Experts have recommended that the LAD should be ligated with tiedto create one to three knots or with a small piece of tubing to compress the coronary artery32,33,34,35,36. In this paper, we suggest a controllable gadget with a snare loop to ligate the LAD in a single suture; this approach enables secure LAD ligation and instant control of loop closure and release while preventing tissue laceration, bleeding, and breaking of the strength of the suture during repeat myocardial puncture, arterial ligation, and ligature release. The approach is, thus, useful for experimental and validation procedures in acute myocardial IR research.
Recognizing anatomical features and histological properties during surgery is helpful for reducing tissue damage and improving study replication. Regarding the opening of the thorax, scholars have suggested separating the pectoral and 3rd or 4th intercostal muscles by using scissors, a retractor, forceps, blunt tweezers, or stitches to pull aside the thoracic muscles and rib cage32,33,35,37,38. The present study suggests an incision along the skin tension lines (the connective tissue framework of the skin)39,40, cutting a single rib's cartilage, which contains avascular flexible connective tissue41, and hooking the thoracic muscle and rib cages to open the chest wall. This approach helps maintain tissue integrity and reduces the bleeding risk. Additionally, starting the approach by identifying reliable surface makers through touch means that the surgical procedure utilizing a skin incision is highly repeatable and consistent.
Confirming the quality of myocardial infarction induced by LAD ligation is a critical step before the investigation of pathophysiological changes in acute myocardial IR research. In the literature, the occurrence of myocardial infarction after LAD ligation is confirmed by observing sudden regional paleness of the myocardium28,33; an acute ST segment of electrocardiogram elevation from the baseline33; elevated serum cardiac enzyme levels such as CK-MB, troponin I, and troponin T28,32,42; or infarcted regions macroscopically42. The consistency of LAD ligation should further be validated by determining the AAR for infarction by using Phthalo or Evan's blue dye32,35,37,38. Low variability in AAR percentage among samples proves the consistency and quality of the procedure for acute myocardial IR research. Moreover, the infarct area can be distinguished from the AAR by demarcating myocardial infarction regions with TTC28,36. Evans blue/TTC double staining was previously employed to evaluate the quality of a myocardial IR study ex vivo37. Compared with the requirement in ex vivo evaluations that the isolated heart be perfused under the Langendorff apparatus, this study supports the animal protocol of in vivo evaluation in which the results are obtained, and the quality of the study is validated instantly and directly.
More importantly, the use of Evan's blue and TTC to define the infarct area to AAR precludes the use of the infarcted myocardium for biochemical analyses, which is a requirement to exclude confounding factors and obtain accurate results in acute myocardial IR research.
Offenlegungen
The authors have nothing to disclose.
Acknowledgements
This model was developed with financial support from the Ministry of Science and Technology, Taiwan (MOST 109-2320-B-030-006-MY3).
Materials
| Evan’s blue | Sigma Aldrich | E2129 | |
| Forceps | Shinva | ||
| Pentobarbital | Sigma Aldrich | 1507002 | |
| Scalpel blades | Shinva | s2646 | |
| Scalpel handles | Shinva | ||
| Silk sutures | SharpointTM | DC-2150N | |
| Surgical needle | AnchorTM | ||
| Triphenyltetrazolium chloride (TTC) solution | Solarbio | T8170-1 | |
| Ventilator | Harvard Rodent Ventilator |
Referenzen
- Khan, M. A., et al. Global epidemiology of ischemic heart disease: Results from the global burden of disease study. Cureus. 12 (7), 9349 (2020).
- Nowbar, A. N., Gitto, M., Howard, J. P., Francis, D. P., Al-Lamee, R. Mortality from ischemic heart disease. Circulation: Cardiovascular Quality and Outcomes. 12 (6), 005375 (2019).
- Kuo, F. Y., et al. Effect of CYP2C19 status on platelet reactivity in Taiwanese acute coronary syndrome patients switching to prasugrel from clopidogrel: Switch Study. Journal of the Formosan Medical Association. , (2022).
- Li, Y. H., et al. Guidelines of the Taiwan Society of Cardiology, Taiwan Society of Emergency Medicine and Taiwan Society of Cardiovascular Interventions for the management of non ST-segment elevation acute coronary syndrome. Journal of the Formosan Medical Association. 117 (9), 766-790 (2018).
- Liu, Y. B., et al. Dyslipidemia is associated with ventricular tachyarrhythmia in patients with acute ST-segment elevation myocardial infarction. Journal of the Formosan Medical Association. 105 (1), 17-24 (2006).
- Anghel, L., Sascău, R., Stătescu, C. Myocardial infarction with cardiogenic shock-the experience of a primary PCI center from North-East Romania. Signa Vitae. 17 (5), 64-70 (2021).
- Samat, A. H. A., Embong, H., Harunarashid, H., Maskon, O. Predicting ventricular arrhythmias and in-hospital mortality in acute coronary syndrome patients presenting to the emergency department. Signa Vitae. 16 (1), 55-64 (2020).
- Wang, Y. C., et al. Outcome of primary percutaneous coronary intervention in octogenarians with acute myocardial infarction. Journal of the Formosan Medical Association. 105 (6), 451-458 (2006).
- Markovic, D., et al. Effects of a percutaneous coronary intervention or conservative treatment strategy on treatment outcomes in elderly female patients with acute coronary syndrome. Signa Vitae. 12 (1), 96-100 (2016).
- Hannan, E. L., et al. Effect of onset-to-door time and door-to-balloon time on mortality in patients undergoing percutaneous coronary interventions for ST-segment elevation myocardial infarction. American Journal of Cardiology. 106 (2), 143-147 (2010).
- McNamara, R. L., et al. Effect of door-to-balloon time on mortality in patients with ST-segment elevation myocardial infarction. Journal of the American College of Cardiology. 47 (11), 2180-2186 (2006).
- Pehnec, Z., Sinkovië, A., Kamenic, B., Marinšek, M., Svenšek, F. Baseline characteristics, time-to-hospital admission and in-hospital outcomes of patients hospitalized with ST-segment elevation acute coronary syndromes, 2002 to 2005. Signa Vitae. 4 (1), 14-20 (2009).
- Menees, D. S., et al. Door-to-balloon time and mortality among patients undergoing primary PCI. The New England Journal of Medicine. 369 (10), 901-909 (2013).
- Ku, H. C., Chen, W. P., Su, M. J. DPP4 deficiency preserves cardiac function via GLP-1 signaling in rats subjected to myocardial ischemia/reperfusion. Naunyn-Schmiedeberg’s Archives of Pharmacology. 384 (2), 197-207 (2011).
- Lee, S. Y., Ku, H. C., Kuo, Y. H., Chiu, H. L., Su, M. J. Pyrrolidinyl caffeamide against ischemia/reperfusion injury in cardiomyocytes through AMPK/AKT pathways. Journal of Biomedical Science. 22 (1), 18 (2015).
- Ku, H. C., et al. TM-1-1DP exerts protective effect against myocardial ischemia reperfusion injury via AKT-eNOS pathway. Naunyn-Schmiedeberg’s Archives of Pharmacology. 388 (5), 539-548 (2015).
- Ku, H. C., Lee, S. Y., Yang, K. C., Kuo, Y. H., Su, M. J. Modification of caffeic acid with pyrrolidine enhances antioxidant ability by activating AKT/HO-1 pathway in heart. PLoS ONE. 11 (2), 0148545 (2016).
- Alonso-Herranz, L., et al. Macrophages promote endothelial-to-mesenchymal transition via MT1-MMP/TGFbeta1 after myocardial infarction. eLife. 9, 57920 (2020).
- Liu, J., Zheng, X., Zhang, C., Zhang, C., Bu, P. Lcz696 alleviates myocardial fibrosis after myocardial infarction through the sFRP-1/Wnt/beta-catenin signaling pathway. Frontiers in Pharmacology. 12, 724147 (2021).
- Goldman, S., Raya, T. E. Rat infarct model of myocardial infarction and heart failure. Journal of Cardiac Failure. 1 (2), 169-177 (1995).
- Ke, J., Zhu, C., Zhang, Y., Zhang, W. Anti-arrhythmic effects of linalool via Cx43 expression in a rat model of myocardial infarction. Frontiers in Pharmacology. 11, 926 (2020).
- Houde, M., et al. Mouse mast cell protease 4 deletion protects heart function and survival after permanent myocardial infarction. Frontiers in Pharmacology. 9, 868 (2018).
- Chen, J., Ceholski, D. K., Liang, L., Fish, K., Hajjar, R. J. Variability in coronary artery anatomy affects consistency of cardiac damage after myocardial infarction in mice. American Journal of Physiology-Heart and Circulatory Physiology. 313 (2), 275-282 (2017).
- Kainuma, S., et al. Influence of coronary architecture on the variability in myocardial infarction induced by coronary ligation in rats. PLoS ONE. 12 (8), 0183323 (2017).
- Heil, J., Schlapfer, M. A reproducible intensive care unit-oriented endotoxin model in rats. Journal of Visualized Experiments. (168), e62024 (2021).
- Schleimer, K., et al. Training a sophisticated microsurgical technique: Interposition of external jugular vein graft in the common carotid artery in rats. Journal of Visualized Experiments. (69), e4124 (2012).
- Lindsey, M. L., et al. Guidelines for experimental models of myocardial ischemia and infarction. American Journal of Physiology-Heart and Circulatory Physiology. 314 (4), 812-838 (2018).
- Li, H., et al. A new model of heart failure post-myocardial infarction in the rat. Journal of Visualized Experiments. (172), e62540 (2021).
- Opitz, C. F., Mitchell, G. F., Pfeffer, M. A., Pfeffer, J. M. Arrhythmias and death after coronary artery occlusion in the rat. Continuous telemetric ECG monitoring in conscious, untethered rats. Circulation. 92 (2), 253-261 (1995).
- Kawashima, T., Sato, F. Clarifying the anatomy of the atrioventricular node artery. International Journal of Cardiology. 269, 158-164 (2018).
- Vikse, J., et al. Anatomical variations in the sinoatrial nodal artery: A meta-analysis and clinical considerations. PLoS ONE. 11 (2), 0148331 (2016).
- Xu, Z., Alloush, J., Beck, E., Weisleder, N. A murine model of myocardial ischemia-reperfusion injury through ligation of the left anterior descending artery. Journal of Visualized Experiments. (86), e51329 (2014).
- Klocke, R., Tian, W., Kuhlmann, M. T., Nikol, S. Surgical animal models of heart failure related to coronary heart disease. Cardiovascular Research. 74 (1), 29-38 (2007).
- De Villiers, C., Riley, P. R. Mouse models of myocardial infarction: Comparing permanent ligation and ischemia-reperfusion. Disease Models & Mechanisms. 13 (11), (2020).
- Reichert, K., et al. Murine left anterior descending (LAD) coronary artery ligation: An improved and simplified model for myocardial infarction. Journal of Visualized Experiments. (122), e55353 (2017).
- Lugrin, J., Parapanov, R., Krueger, T., Liaudet, L. Murine myocardial infarction model using permanent ligation of left anterior descending coronary artery. Journal of Visualized Experiments. (150), e59591 (2019).
- Wu, Y., Yin, X., Wijaya, C., Huang, M. H., McConnell, B. K. Acute myocardial infarction in rats. Journal of Visualized Experiments. (48), e2464 (2011).
- Muthuramu, I., Lox, M., Jacobs, F., De Geest, B. Permanent ligation of the left anterior descending coronary artery in mice: a model of post-myocardial infarction remodelling and heart failure. Journal of Visualized Experiments. (94), e52206 (2014).
- Langer, K. On the anatomy and physiology of the skin. British Journal of Plastic Surgery. 31 (4), 277-278 (1978).
- Carmichael, S. W. The tangled web of Langer’s lines. Clinical Anatomy. 27 (2), 162-168 (2014).
- Chang, L. R., Marston, G., Martin, A. Anatomy, Cartilage. StatPearls. , (2022).
- Kolk, M. V., et al. LAD-ligation: A murine model of myocardial infarction. Journal of Visualized Experiments. (32), e1438 (2009).
