Flow cytometric analysis of single cell suspensions of small-intestinal lymphocytes should yield a discrete population of cells that have similar forward and side scatter characteristics as splenocytes (Figures 1A and 1B). The lymphocytes may begin to die if the tissue is not maintained at 4 °C during the initial stages of the isolation, resulting in the lymphocyte population having a lower forward scatter and being more difficult to separate from other epithelial and dead cells (Figure 1C). Moreover, if the small-intestinal tissue is not completely cleaned of its mesenteric fat, there is virtually a complete loss of lymphocytes (Figure 1D). These features illustrate how working quickly (i.e., not allowing the tissue to warm up) and paying attention to detail (i.e., removing even small amounts of mesenteric fat) is necessary to ensure sample quality. Typically, we obtain ~80% viability for small-intestinal LPLs (Figure 1E).
Figure 2A demonstrates how the composition of the microbiota can greatly affect the numbers of specific cell populations. As we have previously demonstrated, germ-free (GF) mice, which are completely devoid of any microorganisms, have a small-intestinal immune system that is markedly immature as compared to specific pathogen-free (SPF) mice, and colonization of GF mice with a normal mouse microbiota (MMb) results in restoration of the small-intestinal immune system14. In contrast, gnotobiotic mice harboring a normal human microbiota (HMb) — and that have a similar number and diversity of fecal bacteria as MMb mice — have a small-intestinal immune system that is indistinguishable from that of GF mice14.
Taking advantage of the coprophagic nature of mice, co-housing mice together represents a simple, yet powerful method for allowing horizontal transmission of organisms between mice. This approach allows one to test whether the resulting change in the microbiota affects the small-intestinal immune system. As an example, we demonstrated that co-housing HMb mice with MMb mice for 4 weeks resulted in the normalization of the number of CD3+ CD8+ T cells in the SI LP (Figure 2B)14. This result confirms that the differences between MMb and HMb mice observed in Figure 2A is due to variations in the microbiota between these mice — variations that are overcome by co-housing the mice together.
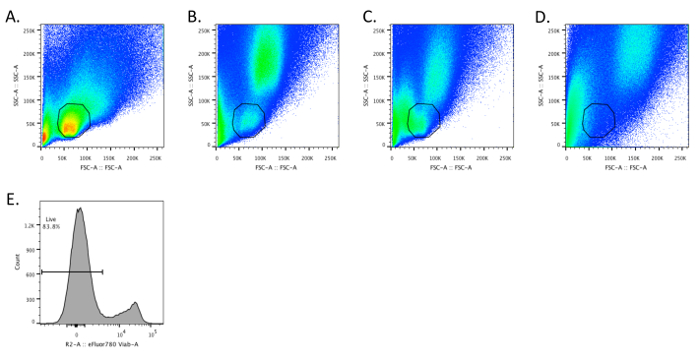
Figure 1. Intestinal Lymphocytes have FSC and SSC Characteristics Similar to Splenocytes. A – D. Dot plots depicting SSC and FSC for optimally prepared splenocytes (A) and small-intestinal lamina propria (SI LP) cells (B – D). B. The SI LP sample was prepared according to the described protocol. C. The intestinal tissue was intentionally allowed to warm to demonstrate that SI LP cells begin to have a lower FSC. D. The mesenteric fat was not cleaned off the small intestine prior to preparing single cells, resulting in the loss of a discernible SI LP lymphocyte population. E. The sample depicted in panel B was stained in step 4.7 with fixable viability dye (e.g., eFluor 780) according to the manufacturer's instructions. Please click here to view a larger version of this figure.
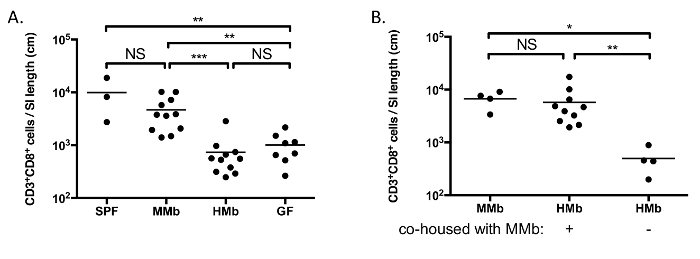
Figure 2. The Microbiota Impacts Maturation of the Small-intestinal Immune System. A. CD3+ CD8+ T cells were enumerated in the SI LP of SPF, MMb, HMb, and GF mice. B. HMb mice were co-housed with MMb mice for 4 weeks prior to enumerating CD3+ CD8+ T cells in the SI LP. MMb and HMb mice that were not co-housed were analyzed for comparison. Each data point represents an individual mouse, and the horizontal bars reflect the mean. NS, not significant; *, p <0.05; **, p <0.01; ***, p <0.001. Figures are reproduced-with permission-from reference 14, with slight modification of B. Please click here to view a larger version of this figure.
