Liver function is primarily assessed by oxygen consumption and flow rate. A flow rate of 4-8 mL/min and oxygen consumption of 1 µmol/min.g is typical. These measures will vary depending on specific experimental conditions and biological differences.
The exact amount of isoflurane used will depend on the type of anesthesia system being used as well as the environment and age/weight of the mouse. During the surgery, the isoflurane and delivery gas do not change, although some changes may be necessary depending on the specifics of the surgical area (e.g., background noise)10. When heparin is injected deep subcutaneously, the onset of action could be delayed by up to 20-40 min. A 10 min waiting period post heparin administration ensures onset of action16. Lidocaine has a 2 min onset of action11.
When inserting the catheter, keep the bevel pointed up, and enter at no more than 15° angle from the portal vein. Both sutures have two knots. The first suture must be tied past the catheter tapper. If cannulation of the portal vein is successful, the liver bleaches from the flush. As the surgeon is resecting the liver, the assistant clears the resected contents with a cotton-tipped applicator. To prevent contaminating the liver and prevent nicks to the lobes, do not cut through the stomach. Do not apply too much tension to the portal vein or liver when holding the catheter to prevent dislodging or tearing the portal vein.
The perfusion hardware setup requires extensive attention to detail (Figure 1). Heparin injections (Figure 2) are essential to the experiment. If blood coagulates, it will occlude the catheter that is inserted into the portal vein, preventing flow. The lidocaine injection (Figure 3) is to aid in desensitizing the area for pain relief. Table 1 provides a simple dosing chart for heparin and lidocaine with saline. The celiotomy and suturing (Figure 4) are essential for a successful portal vein catheterization, liver resection, and successful transfer to the perfusion rig. Flow rate and oxygen consumption measurements are vital to monitoring the liver's health and function (Figure 6). There is often a slight difference in O2 consumption between fed and fasted livers, which we attribute to increased energy demands imposed by gluconeogenesis in the fasted liver.
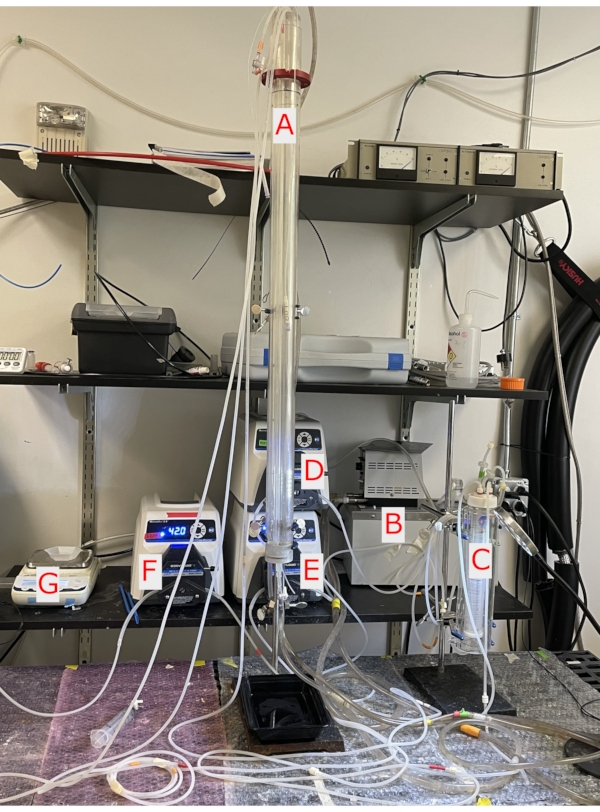
Figure 1. Perfusion column and pumps. A. A 100 cm water-jacketed glass column in which the liver hangs at the bottom. B. The water pump circulates water through the glass column and heats the perfusate. C. Glass thin layer oxygenator is pressurized with 95%/5% O2/CO2 oxygenating the perfusate. D. The ball-bearing pump circulates perfusate from the water bath into the thin layer oxygenator and the glass column. E. The ball-bearing pump circulates perfusate being delivered into the column from the delivery pump keeping perfusate oxygenated and maintaining a flow of 8 mL/min. F. The ball-bearing pump removes efferent perfusate from the NMR tube. G. Weighing scale to weigh perfusate from NMR tube to obtain flow rate of the liver. Please click here to view a larger version of this figure.
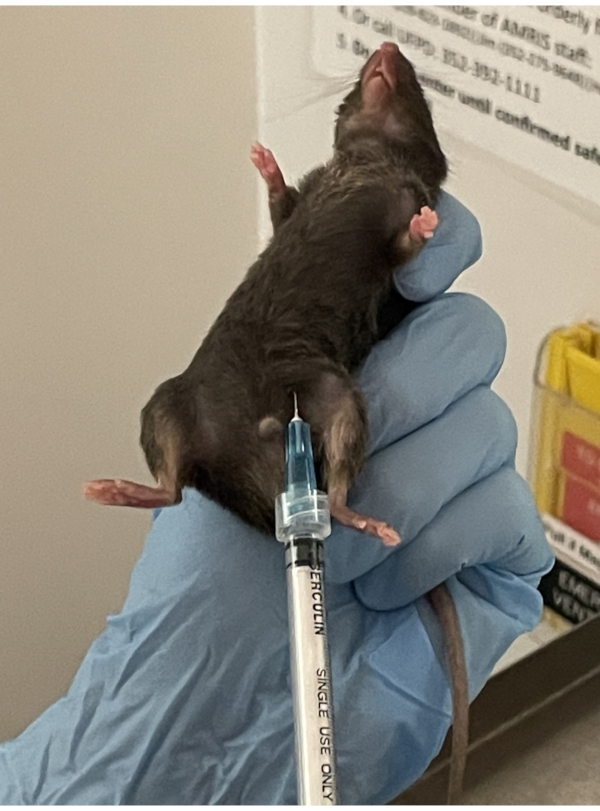
Figure 2. Heparin injection. Deep subcutaneous injection of heparin is given in the lower abdominal fat layer of the mouse. It is important when picking up the mouse, to pull the skin tight to allow the needle to penetrate the skin with ease. Please click here to view a larger version of this figure.
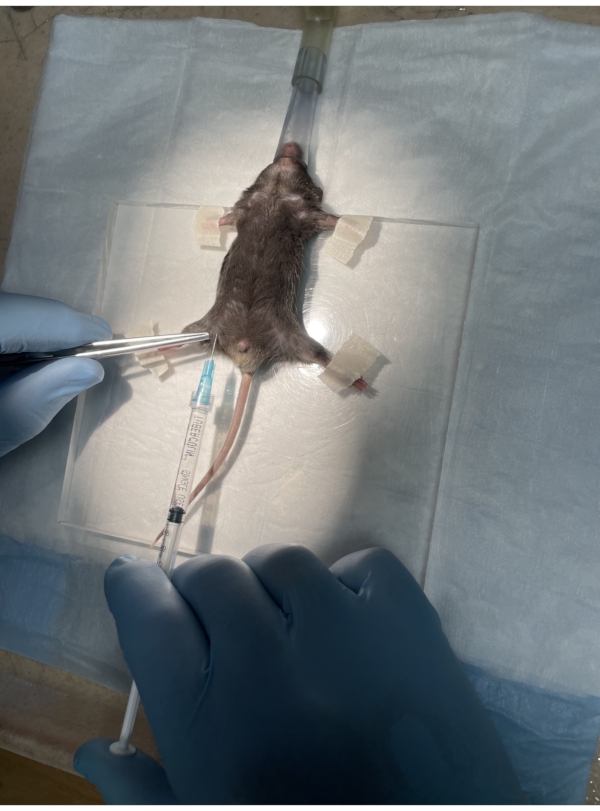
Figure 3. Lidocaine injection. The mouse is placed in the supine position on the surgical platform with its paws taped down and the nose in the nose cone. Lidocaine is administered subcutaneously in the iliac crest region. Please click here to view a larger version of this figure.

Figure 4. Celiotomy and suture. The celiotomy exposes the internal organs, and a hemostat pulls traction through the xiphoid process to help open the incision further. Two sutures are placed around the portal vein, the catheter is inserted, and the sutures are tied. Please click here to view a larger version of this figure.
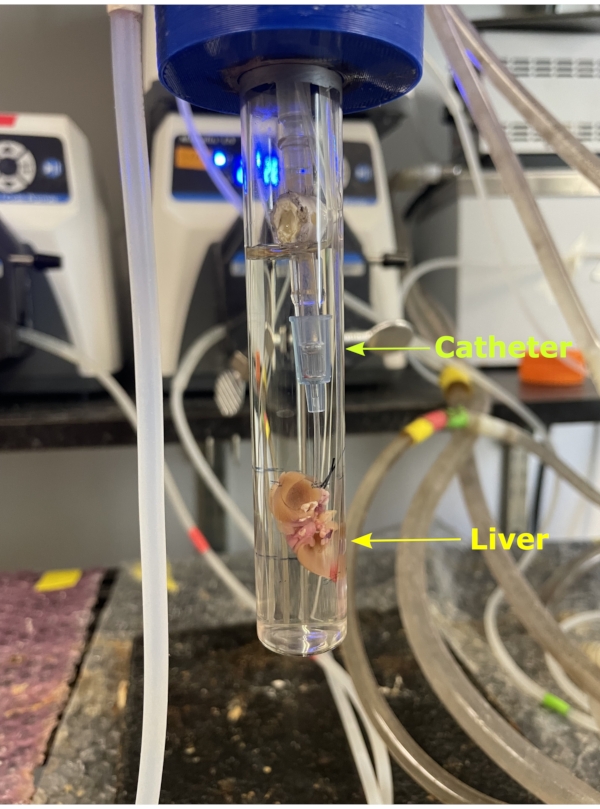
Figure 5. NMR tube. The liver removed from the body along with the catheter which is then attached to the silicon tubing attached to the glass column. The liver is hung from the column and encapsulated by the NMR tube. A 20 mm NMR tube is then carefully screwed onto the column encapsulating the liver. Please click here to view a larger version of this figure.
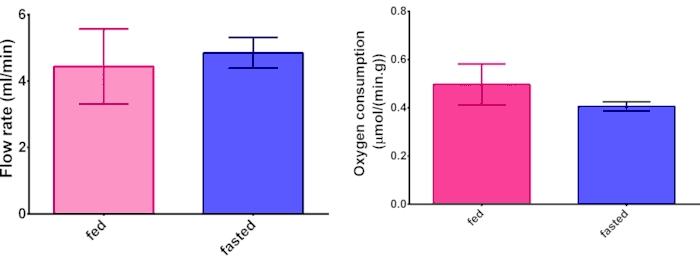
Figure 6. Oxygen consumption and flow rate. Representative data from comparing hepatic oxygen consumption and flow rate measurements between fed and fasted livers. N = 3 and error bars are standard deviation. Please click here to view a larger version of this figure.
| Heparin 1000 units/mL | Saline 0.9% | Total |
| 0.01 mL | 0.19 mL | 0.2 mL |
| Lidocaine 2% | Saline 0.9% | Total |
| 0.2 mL | 0.6 mL | 0.8 mL |
Table 1. Heparin and lidocaine dose with saline. The table displays the concentration of heparin and lidocaine and the dose of each pharmaceutical with saline.
