Human skin xenografts were performed on NSG mice inside a super-barrier animal facility. Success was defined by the prolonged graft and mouse survival and behavioral health of mice post-transplant. Poor survival during the week following surgery was initially observed as the biggest barrier to experimental success, with up to 50% of mice requiring euthanasia. Improving sterile technique and better support of mouse body temperatures during and immediately after surgery increased surgical survival consistently to over 80% and often to 90%-100% survival. While the addition of antibiotics in the mouse drinking water was trialed, it was not determined to improve outcomes and was discontinued as a potential confounder of results. Successfully grafted mice should appear active and healthy in the days following the transplant. Mice were moving around their cage, exploring, building nests, and eating and drinking as usual. An unwell mouse may seem lazy, non-reactive, and may not be eating or drinking enough to maintain its weight. Supplementation of lethargic mice with soft-feed and oral hydration options may assist post-surgical recovery.
A xenograft that is healing correctly will first scab and then recover within about 50 days of surgery. Grafts may contract over time but remain adherent around the edges where the donor skin meets the mouse's skin (Figure 2). While graft scabbing should subside, grafts will remain thicker and more inflamed than healthy human skin (Figure 2). Excessive contraction of grafts can occur, reducing available tissue for endpoint analysis. Utilization of consistently sized grafts and appropriate graft placement is expected to mitigate such issues. All grafts throughout five independent experiments survived to the time of harvest, up to 50 days post-transplant.
Tissue analysis may include immunohistochemistry and single-cell analyses following enzymatic digestion. A portion of skin was processed by overnight digestion in 250 IU/mL of Collagenase Type IV and 0.02 mg/mL of DNase in cell culture media (see Table of Materials), and stained for surface and intracellular markers as previously described14. Analysis by flow cytometry revealed the sustained presence of human immune cells within most grafts but counts varied between xenografts (Figure 3A). Figure 3B shows representative results from a successful graft (left) and one that has failed to maintain human immune cells (right). Analysis of hematoxylin and eosin-stained (H&E) sections taken from the center of the graft revealed intact, non-devitalized skin composed of human dermis and epidermis for both 35 and 50 day time points (Figure 4).
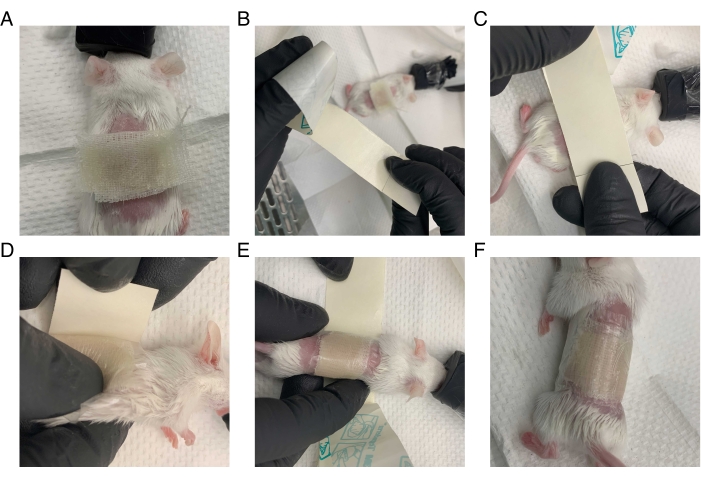
Figure 1: Method for bandaging mouse after surgery. The mouse is wrapped tightly in petrolatum gauze and transparent film dressing while under anesthesia. (A) Petrolatum gauze is placed over an area slightly larger than the surgical wound. (B) The transparent film dressing is prepared: a long strip is cut slightly wider than the petrolatum gauze. The backing covering the adhesive side of the transparent film dressing is partially removed. (C) The adhesive side of the film is firmly pressed against the back of the mouse, leaving an inch of space on the front end of the film. (D) The mouse is turned on its back. The overhanging front portion of the film is pressed onto the mouse, and the backing is removed. (E) The mouse is tightly wrapped in the film, and the remaining support is removed as the mouse is wrapped. (F) The mouse is successfully wrapped in the dressing, and its arms and legs are unconstrained. Please click here to view a larger version of this figure.
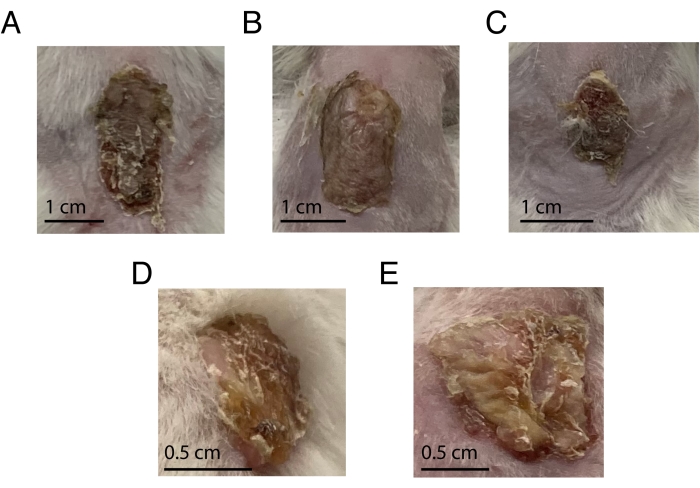
Figure 2: Representative images from transplanted animals from Day 10 to 21 post-transplant. (A–C) Three different mice with optimal transplants at day 10. (D–E) Two different mice with transplants on day 21. Please click here to view a larger version of this figure.
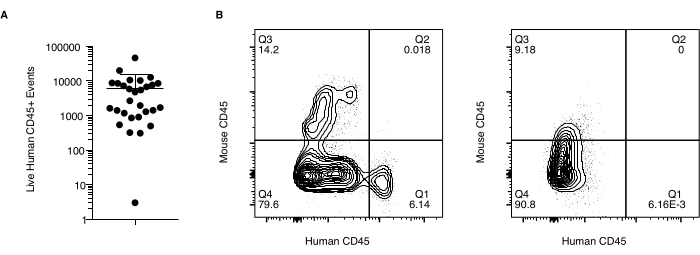
Figure 3: Immune cell chimerism in grafted skin. Flow cytometry data of human immune cell recovery from xenografts. Data is gated on the events of singlet, live, human CD45+ mouse CD45-. (A) Number of cells (Live Human CD45+ Events) recovered from two independent experiments. (B) Representative plots of human and mouse CD45+ immune cell staining in a successful graft (left) compared to graft with unsuccessful maintenance of the human immune compartment (right). Please click here to view a larger version of this figure.
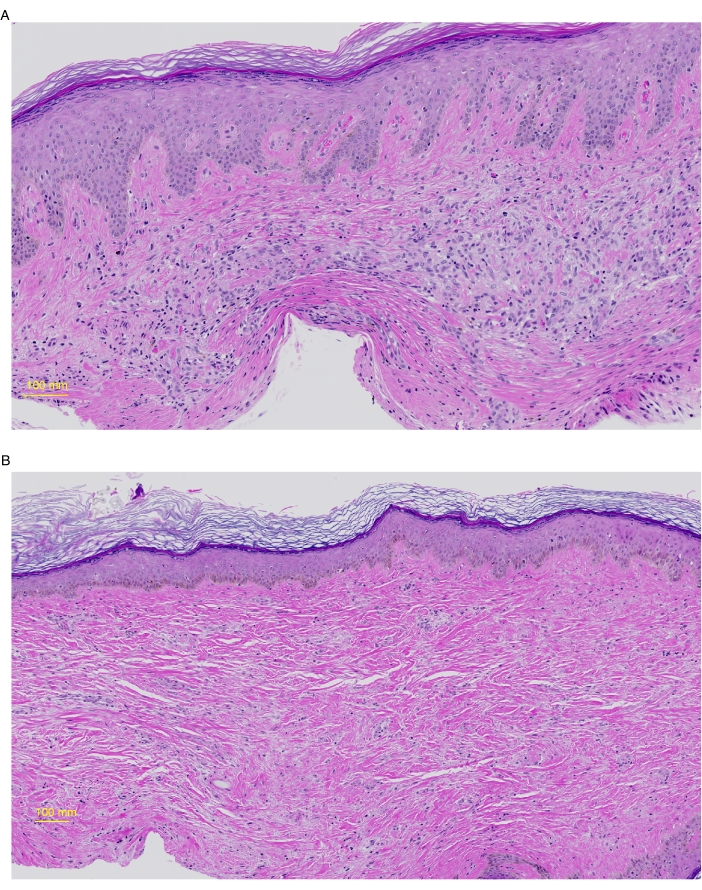
Figure 4: Histology of grafted human skin at day 35 and 50. Grafted skin was harvested from mice on day 35 (A) or 50 (B), preserved in 10% formalin, and paraffin-embedded and stained for Hematoxylin and Eosin (H&E). (A) The epidermis shows moderate hyperplasia (acanthosis), slight hyper-granulosis, and compact orthokeratosis. In the papillary dermis, there are occasional dilated and congested capillaries. Melanocytes and melanin pigment are present in the basal layer of the epidermis. The dermis is moderately cellular and is composed of plump oval fibroblasts with pale syncytial cytoplasm and scattered lymphocytes. (B) The epidermis comprises stratified squamous epithelium, basket-weave orthokeratosis in the cornified layer, and is of normal thickness. Melanocytes and melanin pigment are present in the basal layer of the epidermis. The dermis shows oval fibroblasts and slightly enhanced extracellular matrix deposition. Please click here to view a larger version of this figure.
Supplementary Figure 1: Timeline of the protocol adopted for the xenograft study. Please click here to download this File.
