השיטה הנוכחית של שימור איברים בהשתלת כבד היא לשטוף את עם והאחסון הבא של כבדי תורם בקור (0-4 מעלות צלזיוס) שימור נוזלים (כגון האוניברסיטה ויסקונסין פתרון או פתרון היסטידין-טריפטופן-ketoglutarate). שיטה זו נקראת אחסון סטטי כקר (SCS). למרות שקצב חילוף החומרים של כבדים ב0-4 מעלות צלזיוס הוא נמוך מאוד, יש עדיין ביקוש לרקמת 0.27 μmol חמצן / דקה / g כבד, שלא יכול להיות מסופקת ב1 SCS. השיטה המקובלת של SCS, ולכן, תוצאות במידה מסוימת של פגיעה (נוספת) של כבדי תורם. בעוד סכום זה של פציעת שימור הוא לא בעיה בכבד תורם באיכות טובה, זה יכול להיות גורם קריטי והגבלה בכבדים הכי מוצלח שכבר סבלו במידה מסוימת של פגיעה בתורם. מסיבה זו, כבדים עם איכות לא טובים או תורם קריטריונים מורחב כבדים (ECD) מה שנקרא לעתים קרובות דחו להשתלה כo הסיכוןכישלון שתל המוקדם F נחשב גבוהה מדי. שיעורים גבוהים של תפקוד מתעכב שתל, שאינו תפקיד עיקרי, ומגבלות שאינן בהשקת מרה (NAS) תוארו במקבלי כבדים מתרומה לאחר מות דם (DCD), תורמים או מקבלי שתלי steatotic 2 מבוגרים. NAS הוא אחד גורמים עיקריים לתחלואה ותמותה לאחר השתלה כבד. NAS עלול להתרחש בשני צינורות המרה תורמת חוץ-וintrahepatic ויכול להיות מלווה בבוצת המרה intraductal ושחקנים היווצרות 3,4. למרות שהוא חשב אטיולוגיה של NAS להיות כמה גורמים ופציעת איסכמיה / reperfusion של צינורות המרה בשימור שתל והשתלה זוהתה כ2,5 מנגנון בסיסי גדול. השתלה של שתל DCD זוהתה כאחד מגורמי הסיכון החזקים ביותר לפיתוח NAS. השילוב של תקופה של איסכמיה החמה בתורם DCD, איסכמיה הקרה בשימור איברים, ולאחר מכן reperfusionהוא חשב פגיעה בנמען שתהיה אחראי לפגיעה בלתי הפיכה של דרך המרה, אשר, בשילוב עם יכולת התחדשות לקויה של צינורות המרה, תוצאות בצלקות והיצרות של דרך המרה fibrotic לאחר השתלה כבד 2,5. NAS דווח בעד 30% מהחולים שטופלו בכבד DCD 6-8. זה הפך להיות ברור כי השיטה הנוכחית של SCS של שתלי כבד להשתלה אינה מספיקה לכבדי ECD preinjured כגון אלה מתורמי DCD. יש צורך בשיטות אלטרנטיביות כדי להגדיל ולייעל את השימוש של כבדי ECD להשתלה.
זלוף מכונת (MP) הוא שיטת שימור איברים שעשויים לספק שימור טוב יותר של איברי תורם, בהשוואה לSCS. חבר הפרלמנט יכול להיות רלוונטי במיוחד לשימור שתלי ECD. יתרון חשוב של חבר הפרלמנט הוא האפשרות לספק חמצן לשתל במהלך תקופת השימור. ניתן לבצע MP בטמפרטורות שונות,אשר סווג כהיפותרמיה (0-10 מעלות צלזיוס), subnormothermic (10-36 מעלות צלזיוס) וnormothermic MP (36-37 ° C) (תמ"א). בהתאם לטמפרטורה המשמשת לMP, הסוג של זלוף נוזל צריך להיות מותאם ועם עלייה בחמצן יותר טמפרטורה צריך להיות מסופק. היישום הקליני הראשון של חבר פרלמנט בהשתלת כבד אנושי התבסס על זלוף היפותרמיה ללא חמצון פעיל של 9,10 זלוף הנוזל. במודלים של בעלי חיים, MP היפותרמיה מחומצן (0-10 מעלות צלזיוס) הוכח להיות השפעה מגנה מפני איסכמיה / פציעת reperfusion של כבד שתל 11 ולספק שימור טוב יותר של מקלעת כלי דם peribiliary של המרה לבלוטות 12. Subnormothermic חומץ MP ב 20 ° C או 30 ° C נחקר גם במודלים של בעלי חיים והראה לספק התאוששות קודמת של פונקצית שתל של כבדי DCD, בהשוואה לSCS 13,14. ההיתכנות של חבר פרלמנט מחומץ subnormothermic של כבדים אנושיים הייתה recדיווח ently בסדרה של שבעה כבדי תורם אנושיים מושלכים 15. תמ"א (37 מעלות צלזיוס) מאפשר ההערכה של כדאיות שתל ופונקציונליות לפני השתלת 16,17. בנוסף, חבר הפרלמנט מאפשר לחימום מחדש הדרגתי של שתל הכבד לפני ההשתלה, אשר כבר הוכיח כדי להקל על התאוששות והחייאה של השתל 18.
מכשיר זלוף שימוש בפרוטוקול הנוכחי לזלוף מכונה כבד מאפשר זלוף הכפול (דרך וריד השער והעורק הכבד) באמצעות שתי משאבות צנטריפוגליות, המספקות זרימה רציפה ופורטל זרימת דם פועם. המערכת היא בשליטה בלחץ, המאפשר אוטומטי הסדרת הזרימה דרך כבד, בהתאם להתנגדות intrahepatic. שתי oxygenators קרום סיבים חלול לאפשר לחמצון של שתל הכבד, כמו גם להסרת של CO 2. הטמפרטורה ניתן להגדיר בהתאם לסוג המיועד של MP (טמפרטורות מינימום יור 10 מעלות צלזיוס). זרימה, לחץ וטמפרטורה מוצגים במכשיר בזמן אמת ומאפשר שליטה מתמדת של תהליך זלוף. סט חד פעמי סטרילי חדש של צינורות, מאגר וoxygenators זמין עבור זלוף של כל שתל (איור 1).
המטרה של מאמר זה וידאו היא לספק צעד אחר צעד לפרוטוקול זלוף מכונה normothermic באתרו לשעבר של כבדי תורם אנושיים באמצעות מכונה זו זלוף הכבד חדש שפותחה.
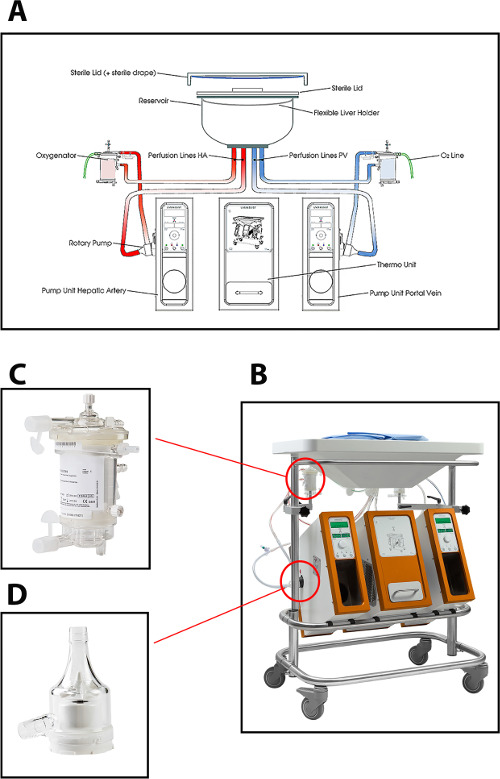
איור 1: (א) ציור סכמטי, (ב) תמונה של המכונה זלוף, (ג) מבט קרוב יותר על oxygenator, ומשאבה צנטריפוגלית משמשת לזלוף normothermic של כבדי תורם אנושיים (ד ').תקבל = "_ blank"> לחץ כאן כדי לצפות בגרסה גדולה יותר של דמות זו.
