The current method of organ preservation in liver transplantation is flush out with and subsequent storage of donor livers in cold (0-4 °C) preservation fluid (such as University of Wisconsin solution or Histidine-Tryptophan-Ketoglutarate solution). This method is referred to as static cold storage (SCS). Although the metabolic rate of livers at 0-4 °C is very low, there is still demand for 0.27 µmol oxygen/min/g liver tissue, which cannot be provided during SCS1. The conventional method of SCS, therefore, results in some degree of (additional) injury of donor livers. While this amount of preservation injury is not a problem in donor livers of good quality, it can become a critical and limiting factor in suboptimal livers that have already suffered some degree of injury in the donor. For this reason, livers with suboptimal quality or so-called extended criteria donor (ECD) livers are frequently rejected for transplantation as the risk of early graft failure is considered to be too high. High rates of delayed graft function, primary non-function, and non-anastomotic biliary strictures (NAS) have been described in recipients of livers from donation after circulatory death (DCD), older donors or recipients of steatotic grafts2. NAS are a major cause of morbidity and mortality after liver transplantation. NAS may occur in both extra- and intrahepatic donor bile ducts and can be accompanied by intraductal biliary sludge and cast formation3,4. Although the etiology of NAS is thought to be multifactorial, ischemia/reperfusion injury of the bile ducts during graft preservation and transplantation has been identified as a major underlying mechanism2,5. Transplantation of a DCD graft has been identified as one of the strongest risk factors for the development of NAS. The combination of a period of warm ischemia in a DCD donor, cold ischemia during organ preservation, and subsequent reperfusion injury in the recipient is thought to be responsible for irreversible injury of the bile ducts, which, in combination with a poor regenerative capacity of the bile ducts, results in fibrotic scarring and narrowing of the bile ducts after liver transplantation2,5. NAS have been reported in up to 30% of patients receiving a DCD liver6-8 . It has become clear that the current method of SCS of liver grafts for transplantation is insufficient for preinjured ECD livers such as those from DCD donors. Alternative methods are needed to increase and optimize the use of ECD livers for transplantation.
Machine perfusion (MP) is a method of organ preservation that may provide better preservation of donor organs, compared to SCS. MP could be especially relevant for the preservation of ECD grafts. An important advantage of MP is the possibility to provide oxygen to the graft during the preservation period. MP can be performed at various temperatures, which have been classified as hypothermic (0-10 °C), subnormothermic (10-36 °C) and normothermic (36-37 °C) MP (NMP). Depending on the temperature used for MP, the type of perfusion fluid has to be adjusted and with increasing temperature more oxygen should be supplied. The first clinical application of MP in human liver transplantation was based on hypothermic perfusion without active oxygenation of the perfusion fluid9,10. In animal models, hypothermic oxygenated MP (0-10 °C) has been shown to have protective effects against ischemia/reperfusion injury of liver grafts11 and to provide better preservation of the peribiliary vascular plexus of the bile ducts12. Subnormothermic oxygenated MP at 20 °C or 30 °C has also been studied in animal models and was shown to provide earlier recovery of graft function of DCD livers, compared to SCS13,14. The feasibility of subnormothermic oxygenated MP of human livers was recently reported in a series of seven discarded human donor livers15. NMP (37 °C) allows for the assessment of graft viability and functionality prior to transplantation16,17. Additionally, MP allows for gradual rewarming of the liver graft before transplantation, which has been demonstrated to facilitate recovery and resuscitation of the graft18.
The perfusion device used in the current protocol for hepatic machine perfusion enables dual perfusion (via the portal vein and the hepatic artery) using two centrifugal pumps, that provide a continuous portal flow and a pulsatile arterial flow. The system is pressure-controlled, allowing auto-regulation of the flow through the liver, depending on the intrahepatic resistance. Two hollow fiber membrane oxygenators allow for the oxygenation of the liver graft, as well as for the removal of CO2. The temperature can be set based on the intended type of MP (minimum temperature of 10 °C). Flow, pressure and temperature are displayed on the device in real-time allowing a continuous control of the perfusion process. A new sterile disposable set of tubing, reservoir and oxygenators is available for the perfusion of each graft (Figure 1).
The aim of this video article is to provide a step by step protocol for ex situ normothermic machine perfusion of human donor livers using this newly developed liver perfusion machine.
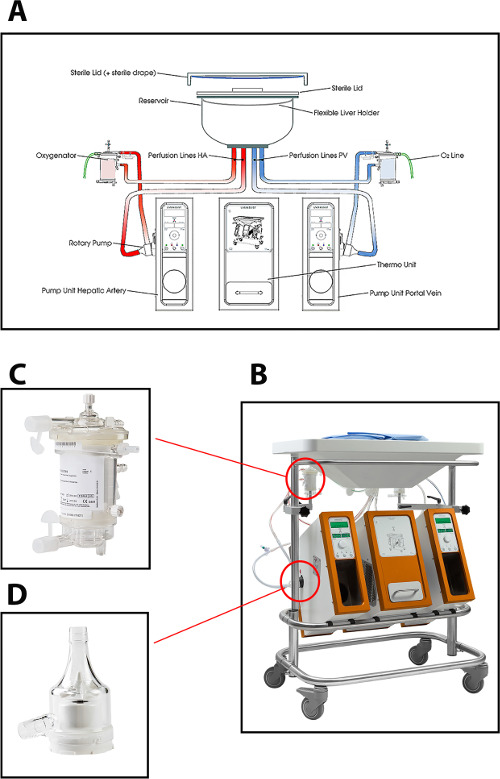
Figure 1: (A) A schematic drawing, (B) a photo of the perfusion machine, (C) a closer view of the oxygenator, and (D) centrifugal pump used for normothermic perfusion of human donor livers. Please click here to view a larger version of this figure.
This protocol has been approved by the Medical Ethical Committee (Medisch Ethische Toetsingscommissie) of the University Medical Center Groningen, the Netherlands.
1. Preparation of the Perfusion Fluid
Note: The total volume of the perfusion fluid prepared for normothermic machine perfusion according to this protocol is 2,233 ml and the targeted osmolarity of the perfusion fluid is 302 mOsmol/L.
- From the components of the perfusion fluid described in Table 1, keep the human packed red blood cells, fresh frozen plasma and human albumin separated. Mix the rest of the components in a sterile manner and store the solution in a sterile bag for transportation to the operating room (OR). Do this in a sterile environment (ideally a Good Manufacturing Practice facility) or in a laminar flow cabinet in a culture room.
| Components | Quantity |
| Packed red blood cell (Hematocrit 60%) | 840 ml |
| Fresh frozen plasma | 930 ml |
| Human albumin 200 g/L (Albuman, Sanquin) | 100 ml |
| Modified parenteral nutrition (Clinimix N17G35E, Baxter International Inc.) | 7.35 ml |
| Multivitamins for infusion (Cernevit, Baxter international Inc.) | 7 μl |
| Concentrated trace elements for infusion (Nutritrace , B. Braun Melsungen AG) | 7.35 ml |
| Metronidazol for i.v. administration (5 mg/ml) (Flagyl, Sanofi-Aventis) | 40 ml |
| Cefazolin 1,000 mg flask 5 ml powder for i.v. administration (Servazolin, Sandoz) | 2 ml |
| Fast-acting insulin (100 IU/ml) (Actrapid®, Novo Nordisk) | 20 ml |
| Calcium glubionate, intravenous solution 10%, 137.5 mg/ml (Sandoz) | 40 ml |
| Sterile H2O | 51.3 ml |
| NaCl 0.9% solution | 160 ml |
| Sodium bicarbonate 8.4% solution | 31 ml |
| Heparin 5,000 IE/ml for i.v. administration | 4 ml |
| Total | 2,233 ml |
Table 1: Components of the perfusion fluid16.
- Transfer human packed red blood cells (840 ml), fresh frozen plasma (930 ml), human albumin 200 g/L (100 ml) and the solution prepared in step 1.1 to the OR to be administered to the perfusion device.
2. Priming of the Perfusion Device
- Add the components of the perfusion fluid, including the human packed red blood cells, fresh frozen plasma, human albumin and the solution prepared in step 1.1 to the machine via the connector on top of the oxygenators and remove all the air bubbles from the tubing.
- Switch on the venous pump and follow the manufacturer’s instructions on the screen. Then turn on the arterial pump and follow the manufacturer’s instructions on the screen.
- Null the pressure meters against atmospheric pressure by following the instructions on the screen. This ensures that the pressure measured during the perfusion is the real pressure at the level of the portal vein and the hepatic artery.
- Start the oxygenation using carbogen (95% O2 + 5% CO2) at a flow rate of 4 L/min. The air flow will be divided among the two oxygenators (2 L/min per oxygenator) and this should result in a pO2 of around 60 kPa (or 450 mmHg) in the perfusion fluid. For longer perfusions, it is advisable to use separate sources of oxygen and carbon dioxide. This allows for small adjustments in the O2/CO2 ratio, which can be used to adjust the pH and pCO2 of the perfusion fluid.
- Take a perfusion sample for blood gas measurement 15-20 min after the device has been primed and monitor the pH and electrolytes accordingly.
NOTE: Be sure to discard about 3 ml of perfusion fluid before taking the samples, as this fluid is in the peripheral tubing and does not represent the perfusion fluid in the system. Add an 8.4% sodium bicarbonate solution for buffering capacity, aiming for a physiological pH (7.35-7.45). For example, add 25-35 ml of an 8.4% sodium bicarbonate solution and check the pH and bicarbonate levels in the perfusion fluid by taking samples for blood gas measurement at regular intervals.
3. Procurement and Preparation of Donor Livers
Note: Procure the organ using the standard technique of in situ cooling and flush out with cold preservation fluid (0-4 °C)19. To facilitate cannulation of the artery, leave a segment of the supratruncal aorta attached to the hepatic artery (Figure 2A).
- Flush out the bile ducts with the preservation fluid (i.e., University of Wisconsin solution). Ligate the cystic duct with a surgical suture.
- Pack and store the organ in a standard sterile donor organ bag and box with crushed ice for subsequent transportation to the MP center.
- Start the back table procedure immediately upon arrival of the donor liver in the operating room.
- Take a sample of at least 10 ml of the preservation fluid for microbiological testing.
- Remove the diaphragmatic attachments to the bare area of the liver as well as any remaining cardiac muscle from the upper cuff of the vena cava with surgical scissors.
- Dissect the artery and portal vein using dissecting scissors and ligate side branches using surgical sutures or hemoclips.
- Close the distal end of the supratruncal aorta segment using a non-absorbable monofilament suture (e.g., 3-0 Prolene). Insert the arterial cannula into the proximal end of the supratruncal aorta and secure with sutures (Figure 2A). Use the cannula provided in the disposable package as supplied by the manufacturer of the perfusion device.
- Insert the venous cannula in the portal vein and secure with sutures. Use the cannula provided in the disposable package. The hepatic vein remains uncannulated.
- Flush out the bile duct with the preservation solution. Insert a silicon catheter into the bile duct and secure with sutures.
NOTE: Do not insert the catheter too deeply into the bile duct as this may cause injury to the biliary epithelium. - Flush out the liver with 0.9% NaCl solution via the portal vein cannula as follows:
- If the graft has been preserved in University of Wisconsin solution as the preservation solution, flush out the liver with 2,000 ml of cold (0-4 °C) 0.9% NaCl solution followed by 500 ml of warm (37 °C) 0.9% NaCl solution.
- If the graft has been preserved in Histidine-Tryptophan-Ketoglutarate solution as the preservation solution, flush out the liver with 1,000 ml of cold (0-4 °C) 0.9% NaCl solution followed by 500 ml of warm (37 °C) 0.9% NaCl solution. The purpose of the warm flush is to prevent a significant drop in the temperature of the perfusion fluid.
- Perform the warm flush immediately before connecting the liver to the perfusion device.
NOTE: Always keep the duration between warm flush and start of NMP less than 1-2 min.
| Donor characteristics (N = 12) | Number (%) or Median (IQR) |
| Age (years) | 61 (50-64) |
| Gender (male) | 8 (67%) |
| Type of donor DCD, Maastricht type III DBD |
10 (83%) 2 (17%) |
| Body mass index (BMI) | 27 (25-35) |
| Reason for rejection DCD+ age >60 years DCD+ high BMI DCD+ various reasons* Severe steatosis |
5 (41%) 3 (25%) 2 (17%) 2 (17%) |
| Preservation solution UW solution HTK solution |
6 (50%) 6 (50%) |
| Donor warm ischemia time in DCD (min) | 14 (17 – 20) |
| Cold ischemia time (min) | 389 (458-585) |
| Donor risk index (DRI) | 2.35 (2.01-2.54) |
Table 2: Donor characteristics. * donor history of intravenous drug abuse for one graft and prolonged donor sO2 <30% after withdrawal of life support for another graft. Abbreviations: DCD, donation after circulatory death; DBD, donation after brain death; UW, University of Wisconsin; HTK, Histidine-tryptophan-ketoglutarate
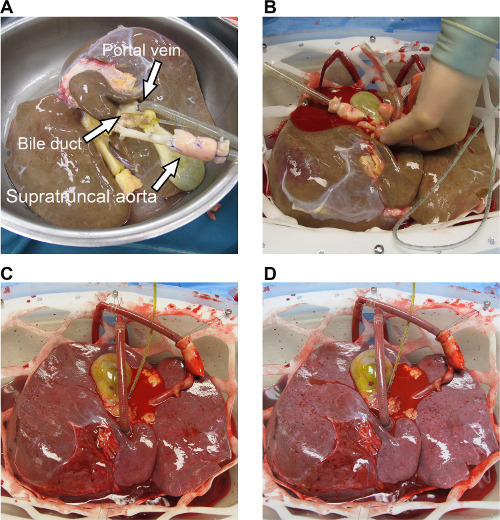
Figure 2: (A) Pictures of a human donor graft that has been prepared on the back table and (B–D) was subsequently perfused normothermically. (A) The arterial cannula is inserted into the surpratruncal aorta and the venous cannula is inserted into the portal vein. The bile duct is cannulated with a silicon biliary catheter. (B) The liver is positioned in the organ chamber with its anterior surface facing downwards and cannulas are connected to the tubings of the perfusion device. (C) 30 min after the start of normothermic machine perfusion. (D) 6 hr after the start of normothermic machine perfusion. During operation the organ chamber is covered by a transparent cover to maintain a sterile moist environment for the liver (not shown in these pictures). Please click here to view a larger version of this figure.
4. Normothermic Machine Perfusion
- Position the liver in the organ chamber with the anterior surface facing downward. Immediately connect the liver to the primed perfusion device by connecting the portal vein cannula to the portal inflow tube of the perfusion device and the arterial cannula to the arterial inflow tube of the device.
- Start perfusion on both portal and arterial side by following the manufacturer’s instructions on the screen. Set the mean arterial pressure at 70 mmHg and the mean portal venous pressure at 11 mmHg.
- Take perfusion fluid samples every 30 min for immediate analysis of blood gas parameters (pO2, pCO2, sO2, HCO2– and pH) and biochemical parameters (glucose, calcium, lactate, potassium and sodium) using a conventional blood gas analyzer. Be sure to discard about 3 ml of perfusion fluid before taking the samples, as this fluid is in the peripheral tubing and does not represent the perfusion fluid in the system.
- To take these samples aspirate the perfusion fluid using a 1 ml syringe from the sampling connectors that are part of the disposable tubing set of the perfusion device. For each sample use a new syringe and immediately remove any air bubbles from the syringe upon aspiration of perfusion fluid. Then insert the syringe in the blood gas analyzer and follow the manufacturer’s instructions provided in the manual of the analyzer.
- Collect plasma from the perfusion fluid, freeze and store at -80 °C for determination of alkaline phosphatase (AlkP), gamma-glutamyl transferase (gamma-GT), alanine aminotransferase (ALT), urea and total bilirubin. Collect plasma after 5 min of centrifugation of the perfusion fluid at 1,500 x g and 4 °C.
12 human livers that were declined for transplantation due to various reasons were used after obtaining informed consent for research from donor families. Donor characteristics are described in Table 2. The human donor livers were perfused normothermically for 6 hr by using the protocol described in this paper. The quality of the liver grafts were evaluated by monitoring the macroscopic homogeneity of liver perfusion (Figure 2A–D). The hemodynamics of the livers were assessed by monitoring the changes in the arterial and portal flows. An initial increase in hepatic artery and portal vein flows and subsequent stabilization of the flows were observed, resulting in a mean arterial flow of 256 ± 16 ml/min (mean ± SEM) and a mean portal vein flow of 748 ± 34 ml/min (mean ± SEM) at 6 hr, indicating stable hemodynamics of livers during perfusion (Figure 3A). Blood gas analysis of the perfusate samples collected from arterial perfusion fluid was used to monitor the status of oxygenation in the perfusion fluid. Oxygenation with carbogen (95% O2 and 5% CO2) at a flow of 4 L/min resulted in a continuous O2 saturation of 100%. Figure 3B displays the oxygenation of the perfusion fluid and subsequent extraction of carbon dioxide in our experience.
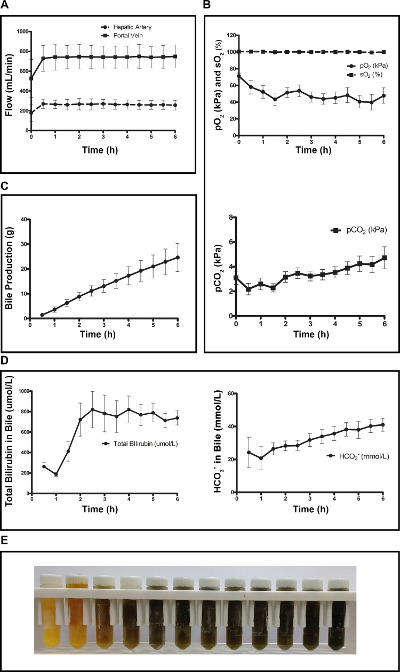
Figure 3: Graphical presentation of perfusion parameters and biochemical analyses of both the perfusion fluid and bile during 6 hr of normothermic machine perfusion of 12 human livers. (A) Changes in arterial and portal flow. (B) Evolution of oxygenation characteristics and pCO2 during 6 hr of normothermic perfusion. (C) Cumulative bile production during perfusion. (D) Increasing concentrations of bilirubin and bicarbonate in bile samples taken during machine perfusion. (E) Microcentrifuge tubes containing bile from a representative graft, demonstrating a gradual darkening shade of the bile color over time. Data are expressed as mean ± SEM. Please click here to view a larger version of this figure.
Bile production was used as an indicator of liver function. Metabolically functioning livers produced bile during NMP, resulting in a mean total bile production of 24.6 ± 6 g after 6 hr of NMP (Figure 3C). An increase in the concentration of total bilirubin and bicarbonate in the bile represented an improvement in the quality of the bile produced during NMP (Figure 3D, E). Liver tissue ATP content as an indicator of mitochondrial function increased during NMP, resulting in mean ATP of 30 ± 5 µmol/g protein (mean ± SEM) after 6 hr of NMP (Figure 4). Biochemical analysis of hepatic injury markers in the perfusion fluid, such as ALT, AlkP, gamma-GT and potassium, was used to assess the amount of graft injury. Stable concentrations of hepatic injury markers reflected minimal injury of the grafts during perfusion (Figure 5A). Lactate and glucose levels in the perfusion fluid as well as oxygen consumption have been described previously17. Furthermore, histological examination of H&E stained biopsies collected from liver tissue and the distal end of the extrahepatic bile duct, as illustrated in Figure 5B, C did not reveal any additional injury to the grafts during normothermic machine perfusion.
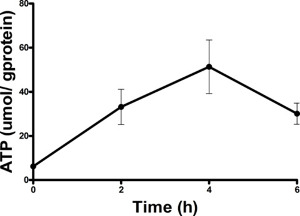
Figure 4: Changes in the level of liver tissue ATP content during NMP. Increased liver tissue ATP content during NMP showed improvement of mitochondrial function. Data are represented as mean ± SEM. Please click here to view a larger version of this figure.
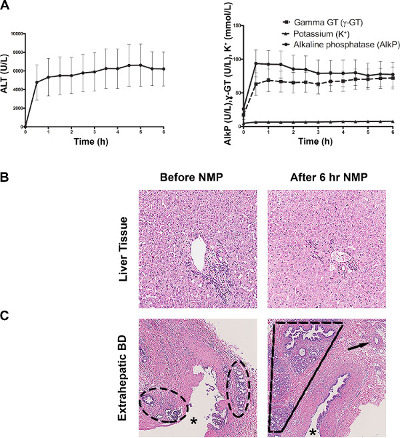
Figure 5: (A) Markers of hepatobiliary injury and (B) staining of liver parenchyma and (C) the extrahepatic bile duct taken from a representative graft before (0 hr) and after (6 hr) machine perfusion. (A) Stable concentrations of injury markers in the perfusion fluid indicated minimal injury of grafts during machine perfusion. (B) Well-preserved microscopic architecture of a representative liver graft. (C) Histology of the extrahepatic bile duct (lumen marked by an asterisk) of a representative graft. Moderate biliary epithelial injury indicated by partial loss of the luminal epithelial layer was observed at baseline and this did not worsen during 6 hr of MP. A similar degree of biliary injury has been described in a series of human livers before transplantation20. Peribiliary vasculature (arrow) and peribiliary glands (area within dashed lines) displayed no worsening of injury after normothermic machine perfusion. Please click here to view a larger version of this figure.
Microbiological testing of the perfusion fluid did not reveal any bacterial contamination during NMP. In one case a positive culture for S. epidermidis was obtained from the sample collected immediately after cold preservation. However, culture of the perfusion fluid after 6 hr of NMP was negative for any bacteria, showing the efficacy of the antibiotics used in the perfusion fluid.
