To investigate change in neurologic function following concussion, baseline and follow-up C3 assessments were analyzed in 181 student-athletes injured during the 2013-2014 athletic seasons. Detailed demographics of the 181 injured athletes are shown in Table 1. Data were stratified into two groups: those who recovered within three weeks of injury (N=92) and those who were still symptomatic three weeks after injury (N=89). When comparing the first post-injury assessments, Welch's two-sample t-tests revealed a significant difference between the two groups for the following C3 app modules: simple reaction time, (P<0.001); choice reaction time, (P<0.001); Trail Making Test B, (P=0.01); and for two of the six BESS stances quantifying postural sway (double limb stance on foam, P=0.02; tandem stance on foam, P=0.04). BESS errors were not significantly different between the two groups, (P=0.26). Results of the analysis are shown in Table 2. These results suggest that athletes who remained symptomatic performed significantly worse on C3 modules measuring information processing, executive function, set switching, and postural stability. Importantly, athletes performed comparably on all modules at baseline (Table 2), and differences were only seen at follow up, suggesting that the modules are effective in detecting change in neurologic function as a result of concussive injuries. Mean performance of the 181 athletes on the C3 modules at baseline and during each post-injury phase of recovery is depicted in Figure 8, stratified by typical versus prolonged recovery.
| Typical | Prolonged | Total | |
| N | 92 | 89 | 181 |
| Age (SD) | 17 (1.29) | 18 (1.31) | |
| Sex, male(%) | 73 (79%) | 66 (74%) | 139 (76.8%) |
| Sport | |||
| Football | 60 | 46 | 106 |
| Soccer | 24 | 30 | 54 |
| Baseketball | 2 | 4 | 6 |
| Volleyball | 1 | 3 | 4 |
| Wrestling | 2 | 2 | 4 |
| Hockey | 1 | 1 | 2 |
| Rugby | 0 | 2 | 2 |
| Altro | 2 | 1 | 3 |
Table 1: Demographic table outlining characteristics of 181 student-athlete diagnosed with concussion.
| BASELINE | FIRST POST-INJURY ASSESSMENT | |||||
| Variable, mean (SD) | Typical | Prolonged | P-Value | Typical | Prolonged | P-Value |
| BESS (total errors) | 14.5 (6.4) | 14.9 (7.2) | 0.65 | 10.9 (5.2) | 11.9 (5.7) | 0.26 |
| Simple Reaction Time | 284.8 (24.4) | 287.6 (25.3) | 0.46 | 294.6 (40.7) | 330.1 (64.7) | 0.0003 |
| Choice Reaction Time | 421.1 (57.7) | 425.7 (60.6) | 0.61 | 403.3 (60.8) | 459.0 (111.9) | 0.0009 |
| Trail Making Test A | 24.2 (8.1) | 23.1 (7.0) | 0.31 | 20.6 (7.1) | 23.4 (8.3) | 0.05 |
| Trail Making Test B | 47.4 (15.7) | 46.7 (16.2) | 0.76 | 38.4 (18.5) | 46.2 (16.2) | 0.01 |
| Processing Speed Test | 58.0 (10.5) | 57.7 (10.2) | 0.81 | 65.0 (11.4) | 62.0 (11.8) | 0.17 |
| Instrumented BESS (CC-PSI percentile) | ||||||
| double limb firm | 46.6 (25.0) | 47.5 (27.4) | 0.83 | 51.6 (23.3) | 42.2 (32.1) | 0.06 |
| single limb firm | 50.0 (22.5) | 53.0 (25.6) | 0.44 | 64.7 (24.8) | 53.4 (31.9) | 0.02 |
| tandem stance firm | 55.6 (26.4) | 54.9 (27.0) | 0.87 | 56.7 (29.1) | 50.5 (26.9) | 0.18 |
| double limb foam | 52.4 (28.7) | 49.7 (28.1) | 0.54 | 57.2 (29.3) | 56.1 (29.5) | 0.82 |
| single limb foam | 55.6 (27.5) | 50.8 (29.6) | 0.29 | 52.9 (32.3) | 46.1 (31.3) | 0.21 |
| tandem stance foam | 40.8 (22.6) | 40.6 (25.3) | 0.96 | 56.7 (28.6) | 47.6 (25.4) | 0.04 |
| Graded Symptom Checklist* | 4.8 (11.2) | 18.4 (20.6) | 0.0001 | |||
| Standardized Assessment of Concussion* | 26.7 (2.5) | 25.8 (4.20 | 0.17 | |||
| *Variables only collected post-injury | ||||||
| Bold indicates significant at P<0.05 | ||||||
| Abbraviations: BESS (Balance Error Scoring System); CC-PSI (Cleveland Clinic Postural Stability Index) | ||||||
Table 2: Results of Welch's two-sample t-tests analyzing differences in performance at baseline (left panel) and at the first follow-up (post-injury) test (right panel) for student athletes who recovered within 21 days of injury (typical recovery) and those who recovered in greater than 21 days (prolonged recovery).
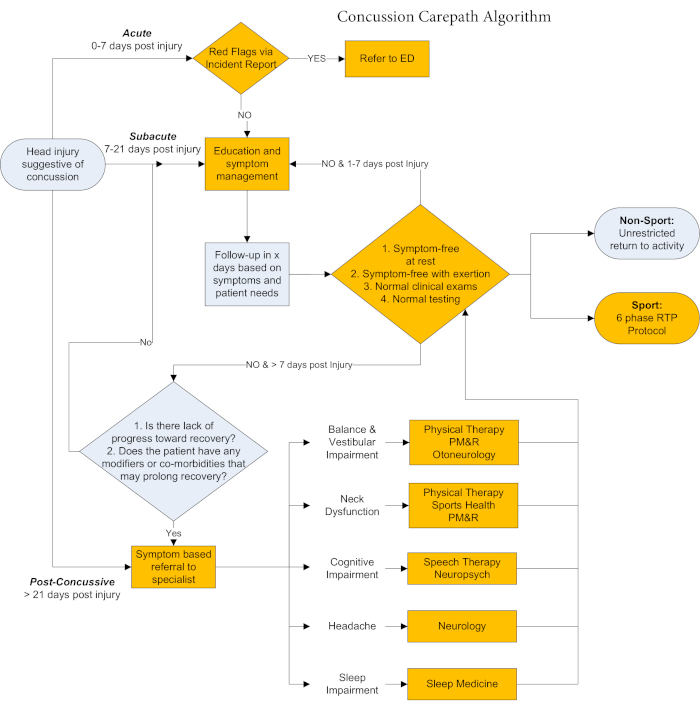
Figure 1: Cleveland Clinic Concussion Carepath algorithm depicting qualifiers guiding clinical care in the acute, subacute, and post-concussive phases post-injury. Fields with gold shading indicate points of care at which standardized, objective outcomes measured through the C3 app integrated with the carepath to guide clinical decision-making. Please click here to view a larger version of this figure.
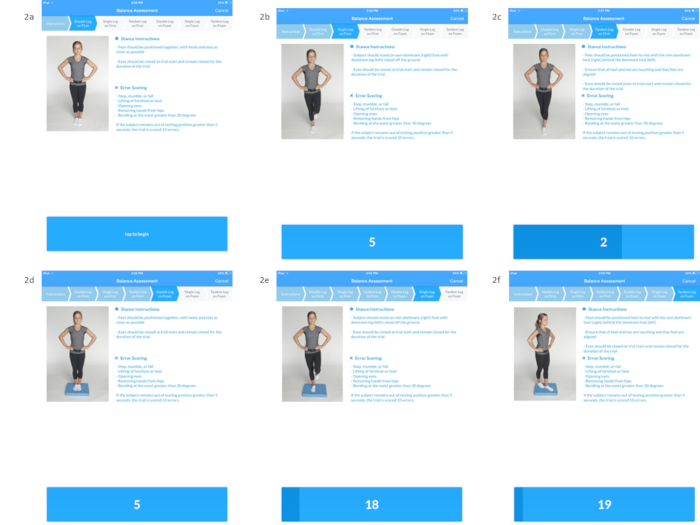
Figure 2: The digital tablet is affixed to the sacrum of the participant to obtain a biomechanical measure of postural sway during performance of the six stances of the Balance Error Scoring System. Double limb stance on firm surface (Figure 2a), Single limb stance on firm surface (Figure 2b), Tandem stance on firm surface (Figure 2c), Double limb stance on foam surface (Figure 2d), Single limb stance on foam surface (Figure 2e), Tandem stance on foam surface (Figure 2f). Please click here to view a larger version of this figure.
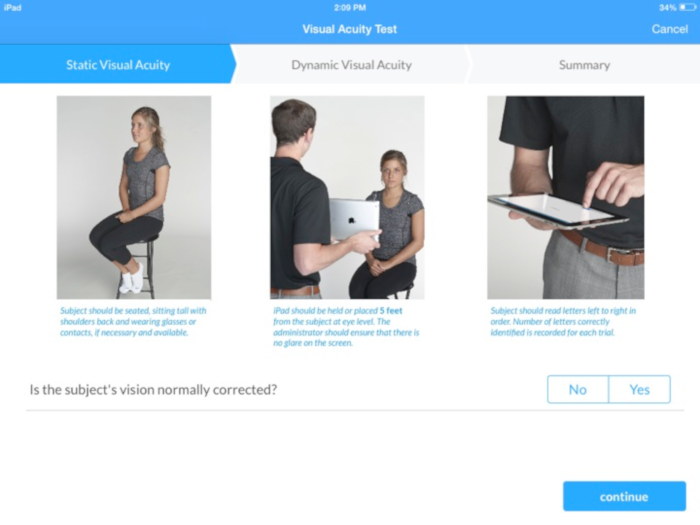
Figure 3: Screen shot depicting instructions for administration of the static visual acuity test. Please click here to view a larger version of this figure.

Figure 4: Screen shots depicting the simple reaction time (Figure 4a) and choice reaction time (Figure 4b) paradigms. Please click here to view a larger version of this figure.
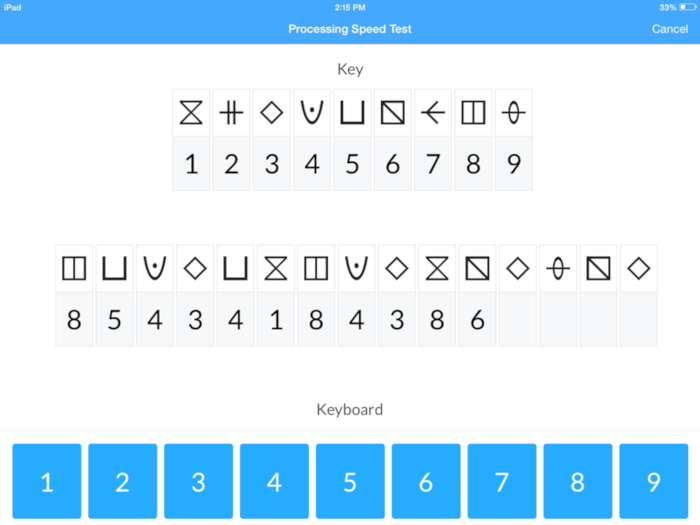
Figure 5: Screen shot depicting the Processing Speed Test (PST). Please click here to view a larger version of this figure.
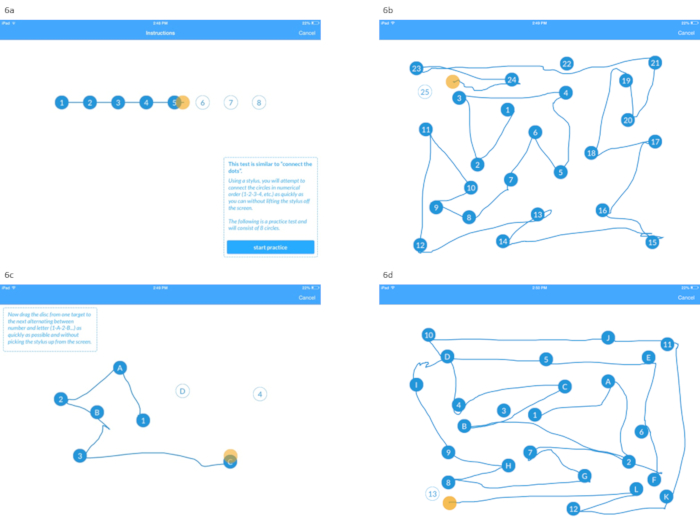
Figure 6: Screen shots depicting the instructions for the Trail Making Test A (Figure 6a) and the digitized Trail Making Test A (Figure 6b), in addition to the Sample Trail Making Test B (Figure 6c), and the digitized Trail Making Test B (Figure 6d). Please click here to view a larger version of this figure.
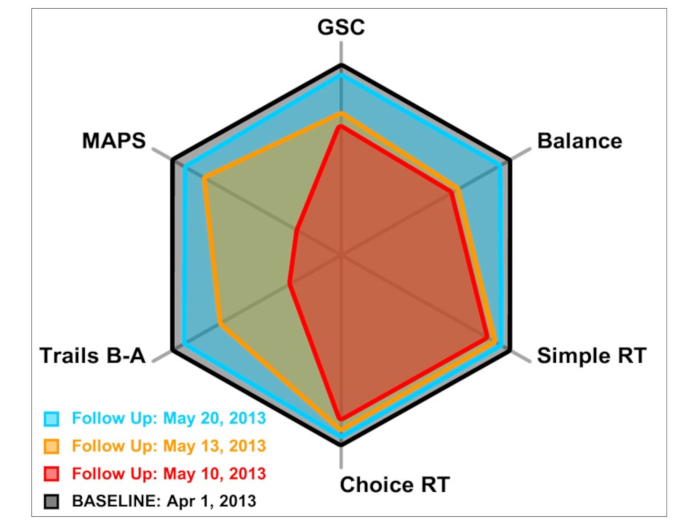
Figure 7: Radar plot depicting baseline and post-injury performance on C3 modules for a representative athlete to aide in C3 app interpretation and guide clinical decision-making. Baseline performance is reflected by the perimeter of the polygon, while the red, yellow, and blue polygons represent performance at 2, 5, and 12 days post-injury, respectively. In the first post-injury assessment, information processing measured by the simple and choice reaction time modules did not appear to be impacted in this patient. However, deficits in balance, processing speed, and in the Trail Making Test were evident. Improvements in all aspects of function measured by the C3 app were evident over the course of recovery, as performance was at or near baseline by 12 days post-injury. Please click here to view a larger version of this figure.
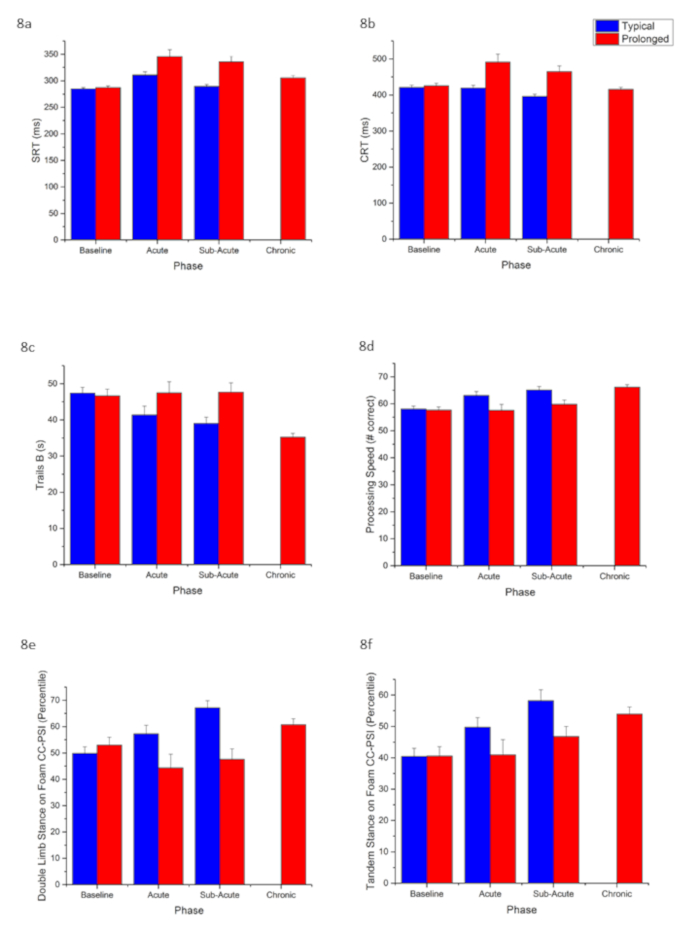
Figure 8: C3 app data for student-athletes (N=181) who incurred a concussion stratified by those who recovered within 3 weeks (typical recovery group, N=92)) and those who took longer than 3 weeks to recover (protracted recovery group, N=89). Bar plots depict mean and standard error of the mean (SEM) performance at baseline and in each phase of recovery post-injury for following C3 app modules: simple reaction time (8a), choice reaction time (8b), Trail Making Test B (8c), Processing Speed Test (8d), Cleveland Clinic Postural Stability Index during BESS double limb stance on foam surface (8e), and Cleveland Clinic Postural Stability Index during BESS tandem stance on foam surface (8f). Please click here to view a larger version of this figure.
