Craniectomy surgery facilitates experimental brain injury and therapeutic cell transplantation: the controlled cortical impact model of brain injury and subsequent cell transplantation therapy require careful removal of the overlying skull. The craniectomy may be performed on any dorsal surface of the skull to permit manipulations to the brain region of interest. The diagram in Figure 1 depicts a 5 mm diameter craniectomy schematic to uncover primary somatosensory and motor cortices (Figure 1A). At 24 h after craniectomy, a second surgery was performed to inject human iPSC-derived neural cell suspension into deep layers of the cortex (Figure 1B). Some cerebral edema is normal on the first day following craniectomy, and particularly after CCI. However, cerebral vasculature sparing during all phases of this procedure is crucial for survival of the cortex. Figure 2 illustrates the cell transplantation procedure in a mouse with minimal cerebral herniation, minimal bleeding, and extensive cortical vascularization. These features are good prognostic indicators of a successful surgery.
Adhesive tape removal testing reveals sensorimotor deficits after unilateral brain injury: the parameters of the brain injury model described above were predicted to affect forelimb sensory and motor function. The adhesive tape removal test was chosen to evaluate the severity of forelimb functional deficits, and the potential therapeutic benefits of cell transplantation. Mice were trained on the testing procedure for 5 days, then allowed to rest for two days prior to baseline behavior testing. Surgeries were performed on the day following baseline testing. Behavior tests in this study were performed on postoperative days 1, 3, 5, 7, 10, 14, 21, 28, 35, and 42. Figure 3 shows results from a pilot experiment in which forelimb function in mice with craniectomy alone (sham) and with CCI injury were compared to forelimb function in naïve mice (n = 11 naïve, 12 sham, 11 CCI). Mice that underwent surgery exhibited transient increased latencies to notice adhesive stimuli for 1-3 days immediately after surgery (Figure 3A,B). Mice showed transient postoperative deficits in adhesive removal from the ipsilateral forepaw as well (Figure 3C). However, mice that underwent CCI exhibited significant deficits in motor performance in the forepaw contralateral to injury compared to naïve mice out to postoperative day 28 (Figure 3D). These data also describe the unexpected severity of sensorimotor loss in craniotomized mice without CCI, indicating that surgical craniectomy to this area also induces TBI-related neurofunctional deficits.
Immunodetection of human induced pluripotent stem cell (iPSC)-derived cell grafts in mouse brain sections: experiments were performed to determine whether human iPSC-derived neural cells would survive long-term transplantation in the mouse brain. Human neural stem cells (NSCs) derived from iPSCs were differentiated into either immature neurons or astrocytes in vitro using established methods17. Transplants of each of the three neural cell phenotypes were tested in our CCI model of traumatic brain injury using the procedure described above and depicted in Figure 2. The mice were euthanized for histologic analysis at 7 days after transplantation. Mouse brain sections were immunostained for the human nuclear antigen (hNA). Human cell grafts could be clearly distinguished from host tissue in sham surgery and CCI brains (Figure 4). Astrocyte grafts (n = 3 sham, 2 CCI) showed poor survival compared to NSCs (n = 12 sham, 15 CCI) and neurons (n = 11 sham, 10 CCI), and were not considered for future experiments.
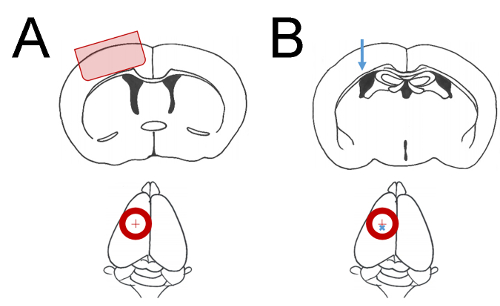
Figure 1: Coordinate parameters of surgical manipulations. Cartoon depictions of mouse brain regions of interest. Red circles indicate a ~5 mm diameter craniectomy. A red cross indicates the craniectomy central point 2 mm lateral to bregma. (A) The shaded region of cerebral cortex in the upper diagram is affected by mild CCI when a craniectomy is performed as shown in lower diagram. (B) The blue arrow in upper diagram indicates the approximate location of cell injections at 1.4 mm depth from cortical surface. The blue cross in the lower diagram indicates the placement of cell injection 2 mm lateral and 1 mm posterior to bregma. Please click here to view a larger version of this figure.
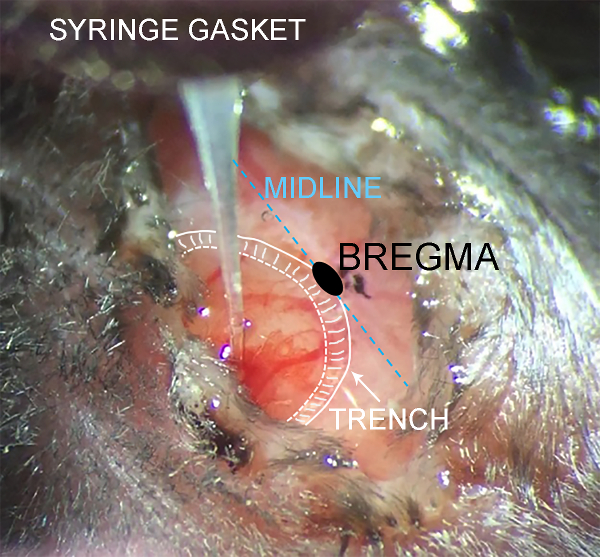
Figure 2: Intraoperative monitoring of cell suspension injection. Photograph taken through a long working distance microscope during intraparenchymal cell injection. Anatomic features are annotated for clarity. The scalp partially obscures the surgery site to minimize dehydration during the procedure. Minor bleeding may occur during needle penetration as shown, which is not cause for concern if large cortical vessels remain intact. Please click here to view a larger version of this figure.
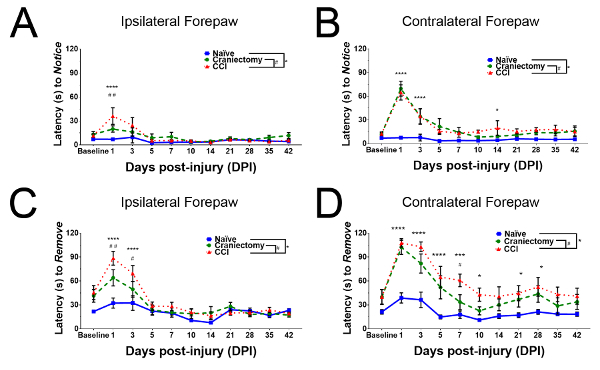
Figure 3: Behavioral evaluation of sensorimotor integration after brain injury. Mice that underwent craniectomy and CCI were compared to naïve controls and to mice that underwent only sham surgery (n = 11 naïve, 12 sham, 11 CCI). Data are presented as group mean latencies, with error bars indicating SEM. (A) Mice that underwent CCI exhibited increased latency to recognize adhesive stimuli applied to the ipsilateral forepaw on the first postoperative day. (B) Mice that underwent craniectomy or CCI exhibited substantially increased latency to notice adhesive stimuli applied to the contralateral forepaw on postoperative days 1 and 3. (C) Mice that underwent craniectomy or CCI exhibited substantially increased latency to remove adhesive stimuli from the ipsilateral forepaw on postoperative days 1 and 3. (D) Mice that underwent craniectomy or CCI exhibited substantially increased latency to remove adhesive stimuli from the contralateral forepaw on postoperative days 1-5. Motor deficits in mice with CCI persisted strongly for 28 days after injury. Please click here to view a larger version of this figure.
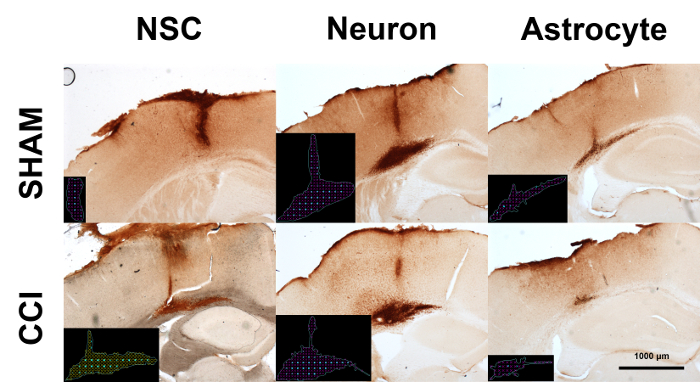
Figure 4: DAB immunohistochemistry for human cell grafts in mouse brains. Human iPSCs were differentiated into neural stem cells (NSCs), neurons, or astrocytes in vitro. Cell cultures were transplanted into mouse brains with or without CCI. Mice were euthanized for histologic analysis seven days after cell transplantation. Micrographs depict representative results of human nuclear antigen staining. Black insets depict markers for stereologic quantification of cell numbers (cyan) and graft volume (red). Please click here to view a larger version of this figure.
