1. Protocol registration
- Register the systemic review.
NOTE: PROSPERO (Table of Materials) was built by National Institute for Health Research for the registration of systematic review. This systemic review protocol has been registered under the number CRD42022301182.
2. Software installation
- EndNote software installation
- Purchase EndNote software and download the exe file as an installation program from EndNote's official website (Table of Materials).
- Decompress the ZIP file. Double-click to start the installer.
- Stata software installation
- Purchase stata software from the Stata official website (Table of Materials).
- Double-click the Stata application program to start the installer.
- TSA software installation
- Go to the website of The Copenhagen Trial Unit (Table of Materials) for registration and downloading a ZIP file.
- Double-click the TSA executable jar file for installation.
3. Database retrieval
- Construct retrieval strategy in the following databases: PubMed, Cochrane Library, Embase, Chinese Biomedical Literature Service System (SinoMed), China National Knowledge Infrastructure (CNKI), Chinese Scientific Journals Database (VIP), and WanFang database (Table of Materials).
- Retrieval time: From the inception of the database to July 2023. Take PubMed as an example:
- Use PubMed advanced search builder (Supplementary Figure 1A).
- Combine the search terms as follows: Angong Niuhuang OR Angong pill OR Bezoar pill) AND (Viral encephalitis.
- Download all the retrieved literature: Send To > Citation Manager > Create File (Supplementary Figure 1B).
4. Inclusion and exclusion criteria
- Inclusion criteria
- Study design: Include randomized controlled trials (RCTs).
- Interventions: Include the comparison between Angong Niuhuang Pill (ANP) plus conventional therapy versus conventional therapy alone.
NOTE: Conventional therapies involved antibiotics, antiviral drugs, intracranial decompression, antipyretics, and maintaining water-electrolyte balance, etc. - Patients: Include patients with viral encephalitis based on the diagnostic criteria.
- Altered mental status: Include patients with no other cause found for altered consciousness, drowsiness, or personality changes lasting ≥24 h.
- Ensure at least 3 of the following associated manifestations are present: (a) Body temperature higher than 38 °C within 72 h before or after onset; (b) Generalized or partial seizures that cannot be entirely attributed to pre-existing epilepsy; (c) New symptoms of neurological defects; (d) White blood cell count ≥ 5/mm2 in cerebrospinal fluid; (e) Neuroimaging showed abnormal brain parenchyma; (f) EEG abnormalities consistent with encephalitis that cannot be attributed to other causes.
- Outcomes: Include outcomes such as total effective rate, time of defervescence, time of consciousness recovery, time of headache disappearance, and time of tic disappearance.
- Exclusion criteria
- Complete the literature retrieval and download the full texts. Read the full texts and exclude studies that meet the exclusion criteria. Record the reasons for each excluded study.
- Additional drug: Exclude studies in which, besides ANP, the treatment group uses additional drugs different from the control group.
- Data missing: Exclude literature with incomplete data.
- Complete the literature retrieval and download the full texts. Read the full texts and exclude studies that meet the exclusion criteria. Record the reasons for each excluded study.
5. Literature management and screening
- Importing literature and removing the duplicates
- Open Endnote and create a new group by clicking My Group > Create Group (Supplementary Figure 2A).
- Import the retrieved literature by clicking on File > Import > Options > Import Options > EndNote Import > Import (Supplementary Figure 2B).
- Remove the duplicates by clicking Reference > Find Duplicates > Keep this Record (Supplementary Figure 2C).
- Screening literature and data extraction
- Create an Excel extraction spreadsheet.
- According to the inclusion and exclusion criteria, have two authors screen the included literature and extract data of included articles independently as follows: 1) first author; 2) publication year; 3) baseline data of a patient with VE (age, gender, ANP usage, duration); 3) outcome measures.
NOTE: Record the reasons for each eliminated study. - Data types: Extract data from dichotomous variables (effective rate), which used sample size and composition ratio, and continuous variables (time of defervescence, time of consciousness recovery, time of headache disappearance, time of tic disappearance), which used mean and standard deviation.
- Create a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart, visualizing the number of studies processed at each step and the reasons for removing them.
6. Quality assessment
- Use the Cochrane risk of bias tool to evaluate the methodology. Include the terms of bias assessment: random sequence generation, allocation concealment, blinding of participants and personnel, incomplete outcome data, selective reporting, blinding of outcome assessment, and other biases.
NOTE: The third party would intervene to resolve discrepancies by discussions.
7. Data synthesis and analysis
- Constructing Forest plots using STATA software
- For continuous data, follow steps 7.1.2-7.1.4.
- For data entry, click User > Meta-Analysis of Binary and Continuous > Main > Continuous. Set the sample size, mean, and standard deviation of the treatment group as n1, mean1, and sd1, and set the sample size, mean, and standard deviation of the control group as n2, mean2, and sd2 (Supplementary Figure 3A).
- Effect model: Appy the effect model (fixed/random) based on I2 statistics among the reported trials. I2 > 50% indicates a high heterogeneity; choose the Random model. Click User > Meta-Analysis of Binary and Continuous > Continuous > Random I-V Heterogeneity. Use Fixed Inverse Variance if I2 ≤ 50%.
- Calculate the outcomes of the same unit as weighted mean difference (WMD); under Estatística, choose noStandard. For different units of outcomes, use the standardized mean difference (SMD); unser Estatística, choose Cohen (Supplementary Figure 3B).
- For dichotomous data, follow steps steps 7.1.6-7.1.7.
- For data entry, use Risk ratios (RR). Click on User > Meta-Analysis of Binary and Continuous > Main > Count. Set the effective number and non-effective number of the treatment group as E1 and NE1, and for the control group as E2 and NE2 (Supplementary Figure 3C).
- Effect model: Apply the effect model (fixed/random) based on I2 statistic among the reported trials. I2 > 50% indicates a high heterogeneity; choose the Random model. Click User > Meta-Analysis of Binary and Continuous > Binary > Fixed. Use Fixed Inverse Variance if I2 ≤ 50%.
NOTE: With small data and few studies, the M-H test is more robust. But M-H can only process binary variables. I-V can be adopted for both continuous and binary variables. - Performing sensitivity analysis using STATA software
- If I2 > 50% in heterogeneity test, perform sensitive analysis to identify the possible cause of heterogeneity. Click on User > Meta-Analysis > influence analysis, metan-based (metainf) > Continuous (Supplementary Figure 3D).
- Checking publication bias using STATA software
- For continuous data, select Egger's linear regression test to assess the publication bias of continuous variables. Use the command db metabias. Click Main, choose _ES _seES, and select Egger (Supplementary Figure 3E).
- For binary data, use RR or OR as the effect indicators of binary variable Harbord's weighted linear regression test. Use the command metabias e1 ne1 e2 ne2, or harbord.
- Trimming and filling procedure using STATA software
- Visualized by a funnel plot, adopt the trim and fill procedure to test the robustness of the effect size estimate to assess publication bias. Use the command db metatrim.
- Click Main and choose _es_sees. Then, click Linear > Fixed > Funnel (Supplementary Figure 3F).
NOTE: Binary variables should make a logarithmic transformation to generate a new dataset for metatrim, such as gen logES = log(_ES).
- Trial sequential analysis
- Build a new meta-analysis. Click on File > New Meta-Analysis. Choose Data Type, import Name, Group1, and Group2 and choose the Outcome Type (Supplementary Figure 4A).
NOTE: For dichotomous data, negative outcome measures such as death, cancer incidence; positive outcome measures such as survival, viral clearance, or smoking cessation. For continuous variables, a negative mean effect increase represents a negative event (e. g., increase in depression score), and a positive mean increase in mean effect is a positive event (e.g., platelet count). - Set effect measure and model according to Forest plot results. Use the Constant continuous correction method and Value = 0.5 (Supplementary Figure 4B).
- Click on Trial, fill in the Study, Year, and Effect and Total number of Intervention and Control groups. Then, click Add Trial (Supplementary Figure 4C).
NOTE: Supplementary Figure 4D shows the data entry tab that is used to distinguish between continuous and binary variables. - Click Tsa > Alpha-Spending Boundary. Set Boundary Type as Two-Sided, the Tipo
 Error rate α = 0. 05 and Power = 0.80. Click Perform Calculation, then Graph to see the figure.
Error rate α = 0. 05 and Power = 0.80. Click Perform Calculation, then Graph to see the figure. - For the meta-analysis of dichotomous outcome, fill the expected event rate and intervention effect, including Relative Risk Reduction (RRR) and Incidence in the control group. According to precious forest plot of total effective rate, calculate RRR (Supplementary Figure 4E).
- For continuous data, click Meta-analysis and choose Mean difference and Randon-effect(BT) according the previos results of forest plot.
- Click on Trial, fill in the Study, Year, Mean response, Standard Deviation and Group size of Intervention and Control groups. Then, click Add Trial.
- Click on Tsa. Select Alpha-Spending Boundary. Then, setting the Boundary Type as Two-Sided, the Type ⅠError rate α to 0.05 and Power to 0.8. Choose Empirical in mean difference and variance.Click Perform Calculation, then click Graph to see the figure.
- Build a new meta-analysis. Click on File > New Meta-Analysis. Choose Data Type, import Name, Group1, and Group2 and choose the Outcome Type (Supplementary Figure 4A).
Search results and study characteristics
Systematic retrieval yielded 122 studies and manual searching added 9 relevant literatures. After removing 49 duplicates, 82 studies remained to be screened by abstract and full-text. Ultimately, 13 studies12,13,14,15,16,17,18,19,20,21,22,23,24 involving 1045 cases were included for meta-analysis (Figure 1). The characteristics of eligible studies are summarized in Table 1. These trials were published in China from 1997 to 2023. All cases with VE were children whose basic data had no significant difference. In terms of the risk of bias, all included studies were suboptimal (Table 2). Only 4 studies had a low risk in random sequence generation, and no trial reported allocation concealment. All studies had complete outcome data. Both blinding and selective outcome reporting of included studies were unclear.
Outcome comparison
Total effective rate
The total effective rate was reported as the primary outcome in 11 studies12,13,14,16,17,18,19,20,21,22,24. As shown in Figure 2A, the total effective rate of adjuvant treatment with ANP was 17% higher than conventional treatment (RR = 1.17, 95% CI[1.08,1.27], I2 = 13.3%, P = 0.00). Harbord's test (P = 0.56) suggested that there was no publication bias (Figure 2B). For RIS, the relative risk reduction (RRR) was set as -17% and the relative event rate of the control group was set as 80%. As shown in Figure 2C, the cumulative Z curve crossed the conventional boundary value and RIS, which indicated that the total effective rate of adjuvant treatment with ANP was significantly higher than conventional therapy and met the requirement of sample size.
Time of defervescence
The time of defervescence for evaluation was reported in 11 studies12,13,14,15,16,17,18,19,20,23,24. Forest plot (Figure 3A) showed that the time of defervescence in adjuvant treatment with ANP was significantly shorter than in conventional treatment (WMD = -1.59, 95% CI[-2.09,-1.09], I2 = 92.1%, P = 0.00). The high heterogeneity is possibly attributed to Yu's23 and Fu's16 studies (Figure 3B). The continuous variable adapted Egger's test for publication bias assessment, P=0.03, which indicated that the outcome referred to publication bias (Figure 3C). However, the trim and fill procedure did not process data, implying the pooled WMD of time of defervescence was robust (Figure 3D). The time of defervescence of adjuvant treatment with ANP was significantly less than conventional therapy and met the requirement of sample size(Figure 3E).
Time of consciousness recovery
The time of consciousness recovery was reported in 8 studies12,13,14,15,16,17,19,20. Forest plot (Figure 4A) showed consciousness recovery was 1.79 days faster in adjuvant treatment with ANP than in conventional treatment (WMD = -1.79, 95% CI[-2.06, -1.51], I2 = 61.9%,P = 0.00). Sensitivity analysis revealed that Zhao's13 study was a noteworthy factor causing high heterogeneity (Figure 4B). No publication bias was verified (P = 0.70) (Figure 4C).
Time of headache disappearance
The time of headache disappearance was reported in 6 studies12,13,15,16,17,20. Figure 5A shows as a forest plot, the time of headache disappearance of adjuvant treatment with ANP was significantly shorter than conventional treatment (WMD = -1.51, 95% CI[-1.93, -1.08], I2 = 80.5%, P = 0.00). Wang's12 study could be the possible cause of high heterogeneity via sensitivity analysis (Figure 5B).
Time of tic disappearance
The time of tic disappearance was reported as an outcome measure in 6 studies13,14,15,19,20,23. Figure 6A showed adjuvant treatment with ANP could significantly shorten the time of tic disappearance than conventional treatment (WMD = -1.88, 95% CI[-2.39, -1.36], I2 = 86.6%, P = 0.00). Sensitivity analysis implied high heterogeneity could be due to the studies of Zhao13 and Yu23 (Figure 6B).
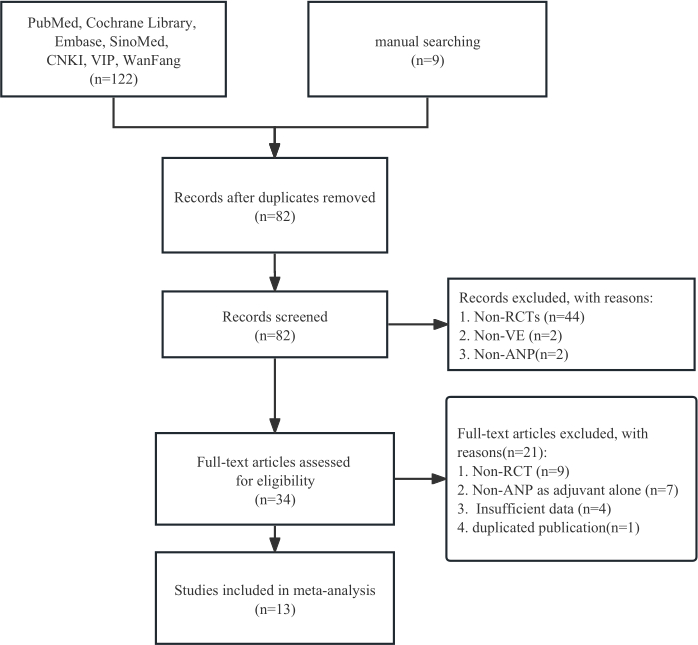
Figure 1: Flow chart of meta-analysis. Please click here to view a larger version of this figure.
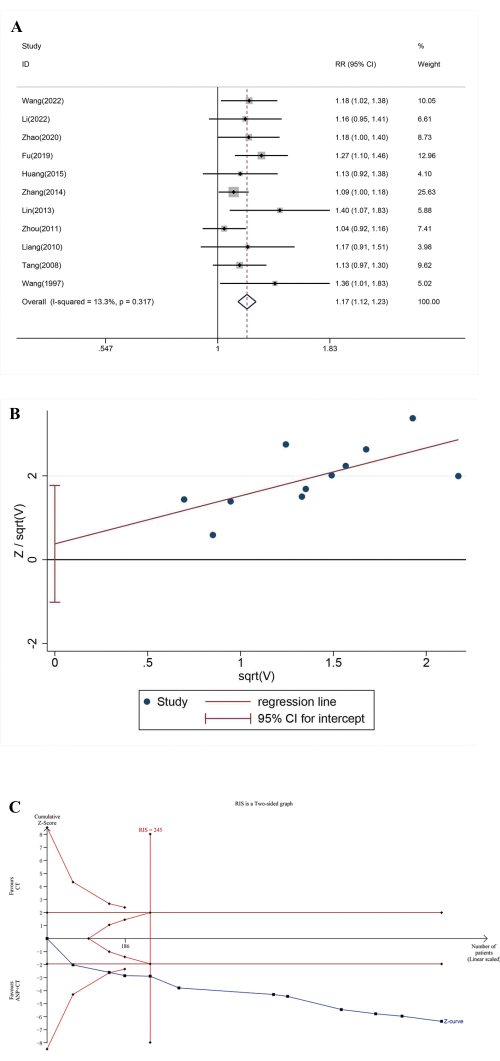
Figure 2: Total effective rate analysis. (A) Forest plots. (B) Publication bias assessment. (C) Trial sequential analysis. Please click here to view a larger version of this figure.
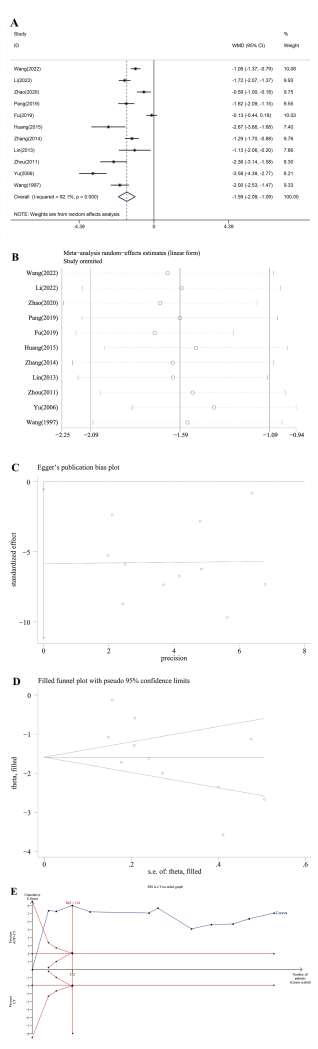
Figure 3: Analysis of time of defervescence. (A) Forest plots, (B) sensitivity analysis, (C) Publication bias assessment, (D) trim and fill procedure, and (E) trial sequential analysis. Please click here to view a larger version of this figure.
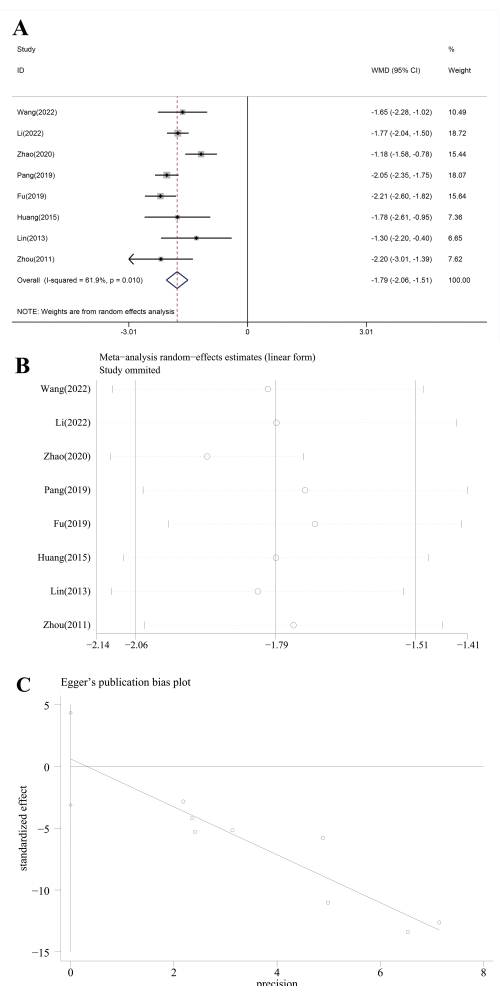
Figure 4: Analysis of time of consciousness recovery analysis. (A) Forest plots, (B) sensitivity analysis, and (C) Publication bias assessment Please click here to view a larger version of this figure.
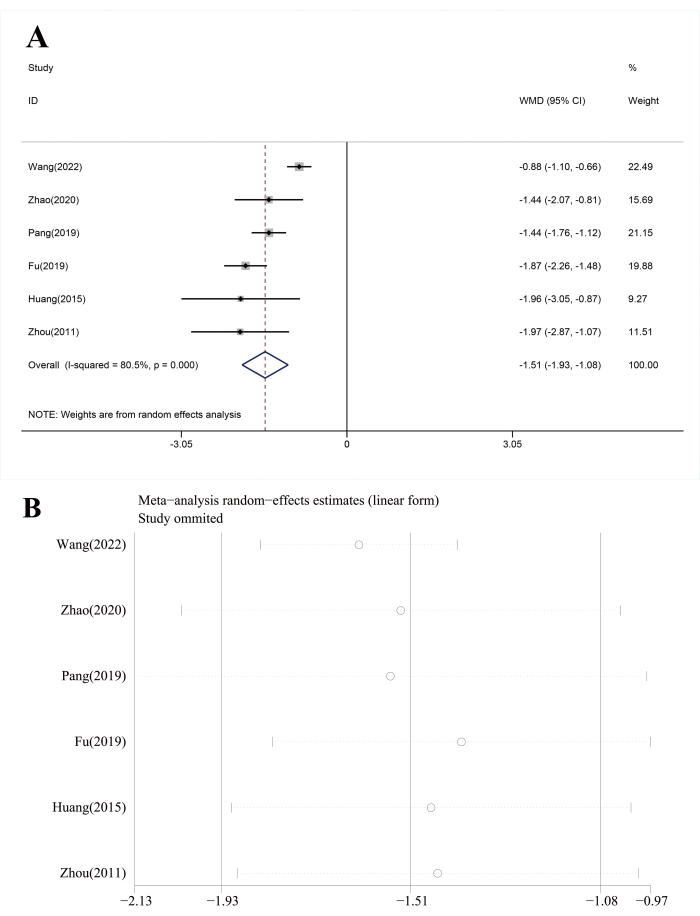
Figure 5: Analysis of time of headache disappearance. (A) Forest plots, and (B) sensitivity analysis. Please click here to view a larger version of this figure.
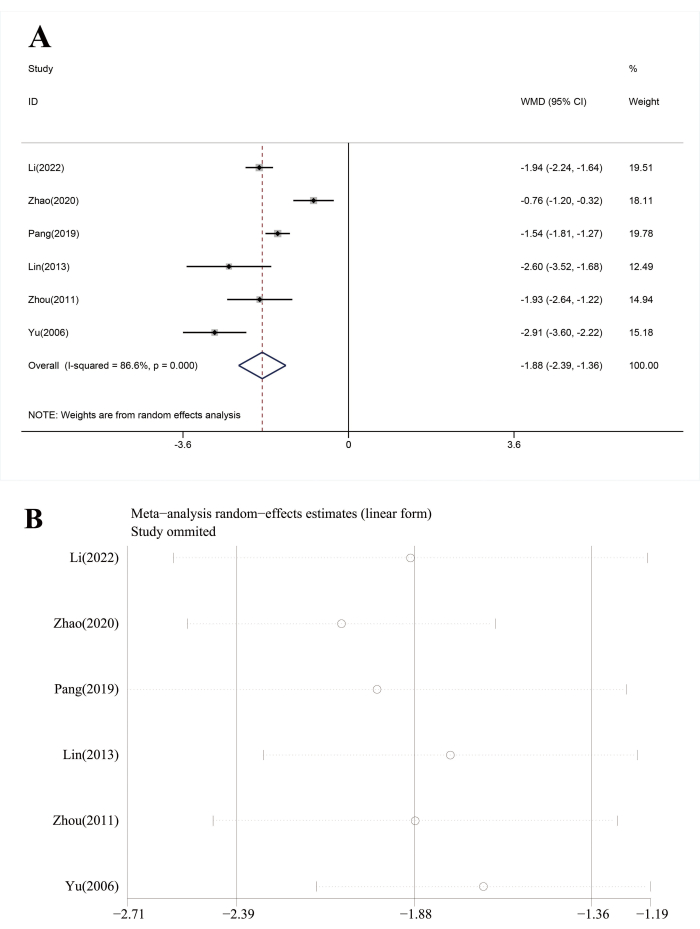
Figure 6: Analysis of time of tic disappearance. (A) Forest plots, and (B) sensitivity analysis. Please click here to view a larger version of this figure.
Table 1: Basic characteristics of included studies.  T: Treatment;
T: Treatment;  C: control;
C: control;  CT: conventional therapy;
CT: conventional therapy;  IG: immune globulin;
IG: immune globulin;  MGS: Monosialotetrahexosyl ganglioside Sodium;
MGS: Monosialotetrahexosyl ganglioside Sodium;  Effective rate;
Effective rate;  Disappearance of headache (day);
Disappearance of headache (day);  Time to defervescence (day);
Time to defervescence (day);  Recovery of consciousness (day);
Recovery of consciousness (day);  Disappearance of motor tics (days). Please click here to download this Table.
Disappearance of motor tics (days). Please click here to download this Table.
Table 2: Risk of bias assessment Please click here to download this Table.
Supplementary Figure 1: Search examples in the PubMed database. (A) The main window of literature retrieval builder in PubMed. (B) The main window for downloading all the retrieved literature. Please click here to download this File.
Supplementary Figure 2: Literature management in Endnote. (A) The main window for creating a new group is (B) The main window of importing the retrieved literature. (C) The main window for removing duplicates. Please click here to download this File.
Supplementary Figure 3: Meta-analysis in Stata. (A)The main window for data entry of forest plots of continuous data. (B) The main window for choosing the model and statistics of continuous data. (C) The main window for data entry of forest plots of dichotomous data. (D) The main window for choosing the model and statistics of dichotomous data. (E) The main window for Egger's test. (F) The main window for the trim and fill procedure. Please click here to download this File.
Supplementary Figure 4: TSA analysis. (A) The main window for creating a new meta-analysis file. (B) The main window for setting effect measure, model, and zero event handling. (C) The main window for adding studies. (D) The different requirements of continuous and dichotomous data. (E) The main window for adding parameters in TSA analysis. Please click here to download this File.
