A Murine Model of Hyperlipidemia-Induced Heart Failure with Preserved Ejection Fraction
Summary
This protocol presents a detailed approach to replicating a murine model of hyperlipidemia-induced heart failure with preserved ejection fraction (HFpEF). The design combines the administration of adeno-associated virus 9-cardiac troponin T-low-density lipoprotein receptor (AAV9-cTnT-LDLR) and poloxamer-407 (P-407).
Abstract
The pathophysiology of heart failure with preserved ejection fraction (HFpEF) driven by lipotoxicity is incompletely understood. Given the urgent need for animal models that accurately mimic cardio-metabolic HFpEF, a hyperlipidemia-induced murine model was developed by reverse engineering phenotypes seen in HFpEF patients. This model aimed to investigate HFpEF, focusing on the interplay between lipotoxicity and metabolic syndrome. Hyperlipidemia was induced in wild-type (WT) mice on a 129J strain background through bi-weekly intraperitoneal injections of poloxamer-407 (P-407), a block co-polymer that blocks lipoprotein lipase, combined with a single intravenous injection of adeno-associated virus 9-cardiac troponin T-low-density lipoprotein receptor (AAV9-cTnT-LDLR). Extensive assessments were conducted between 4 and 8 weeks post-treatment, including echocardiography, blood pressure recording, whole-body plethysmography, echocardiography (ECG) telemetry, activity wheel monitoring (AWM), and biochemical and histological analyses. The LDLR/P-407 mice exhibited distinctive features at four weeks, including diastolic dysfunction, preserved ejection fraction, and increased left ventricular wall thickness. Notably, blood pressure and renal function remained within normal ranges. Additionally, ECG and AWM revealed heart blocks and reduced activity, respectively. Diastolic function deteriorated at eight weeks, accompanied by a significant decline in respiratory rates. Further investigation into the double treatment model revealed elevated fibrosis, wet/dry lung ratios, and heart weight/body weight ratios. The LDLR/P-407 mice exhibited xanthelasmas, ascites, and cardiac ischemia. Interestingly, sudden deaths occurred between 6 and 12 weeks post-treatment. The murine HFpEF model offers a valuable and promising experimental resource for elucidating the intricacies of metabolic syndrome contributing to diastolic dysfunction within the context of lipotoxicity-mediated HFpEF.
Introduction
Heart failure with preserved ejection fraction (HFpEF) denotes a cardiometabolic syndrome accompanied by multiple comorbidities and constitutes over 50% of all heart failure cases1,2. Moreover, the frequency of HFpEF has steadily risen over the past decade3. With limited treatment options, HFpEF represents the most significant unmet medical necessity in cardiovascular disease, given its multifaceted pathophysiology4. Thus, an urgent need exists to enhance comprehension of the underlying mechanisms and pathophysiology of HFpEF to develop effective therapies.
Despite significant advancements in recent years, the pathophysiology of HFpEF attributed to lipotoxicity remains incompletely understood. It is established that patients with HFpEF exhibit notable myocardial lipid accumulation compared to those with heart failure with reduced ejection fraction (HFrEF) and healthy controls5. RNA sequencing data from cardiac biopsies showed downregulation of the lipoprotein lipase (LPL) gene in the HFpEF group compared to the healthy and HFrEF patients6. Poloxamer-407 (P-407) is a block co-polymer that induces hyperlipidemia by blocking LPL and subsequently increasing plasma triglycerides and low-density lipoprotein (LDL) cholesterol7. Previous studies demonstrated high LDL-Receptor (LDLR) expression in the hearts of HFpEF mice8.
Building upon these findings and recognizing the pressing need for animal models accurately mimicking cardio-metabolic HFpEF, a hyperlipidemia-induced murine model was developed and presented. This model was tailored to explore HFpEF, explicitly focusing on the involvement of lipotoxicity alongside metabolic syndrome. Induced by hyperlipidemia/LPL blockade and enhanced cardiac LDLR expression, this model was established in WT-129 mice on 129J background through biweekly intraperitoneal (i.p.) injections of P-407 combined with a single intravenous (i.v.) injection of adeno-associated virus 9-cardiac troponin T-LDLR (AAV9-cTnT-LDLR)9.
Between 4 and 8 weeks post-treatment, an extensive array of assessments was conducted, encompassing echocardiography, blood pressure recordings, whole-body plethysmography (WBP), continuous electrocardiography (ECG) telemetry, activity wheel monitoring (AWM), as well as biochemical and histological analyses9. At four weeks, the LDLR/P407 or “double treatment” mice exhibited distinct HFpEF features, including diastolic dysfunction, preserved ejection fraction, and increased left ventricular wall thickness9. Additionally, ECG telemetry and AWM revealed heart blocks and reduced activity, respectively. Notably, blood pressure and renal function remained normal9. By eight weeks, diastolic function deteriorated, and WBP measurements unveiled reduced respiratory rates9.
Further exploration of the double treatment model revealed fibrosis, elevated wet/dry lung ratios, and heart weight/body weight ratios9. Necropsy revealed ascites, cardiac ischemia, and xanthelasmas. Intriguingly, sudden deaths were documented between 6 and 12 weeks post-treatment9. This murine hyperlipidemia-driven HFpEF model provides a rapid, valuable, and promising experimental tool for unraveling the complexities of metabolic syndrome contributing to diastolic dysfunction with lipotoxicity-mediated HFpEF.
Protocol
The animal protocol was approved by the Institutional Animal Care and Use Committee (IACUC) at the University of Miami, conforming to National Institute of Health (NIH) guidelines (IACUC protocol 23-103-ad03). For the present study, wild-type (WT) mice on 129J background were acquired from a commercial source (see Table of Materials) and bred in-house. All mice were littermates on 129J background. Experiments included both male and female mice. The LDLR/P-407 HFpEF mouse was established by administering a single dose of AAV9-cTnT-LDLR at week one and bi-weekly p407 for four weeks.
1. AAV9-cTnT-LDLR preparation and administration
NOTE: AAV9-cTNT-hLDLR plasmid (see Table of Materials) encodes the full human LDLR protein (2664bp) (Figure 1).
- AAV-LDLR viral vector preparation
- Based on the number of animals, thaw AAV9 stock vials on ice for 20 min, then dilute AAV particles in Dulbecco’s Phosphate Buffered Saline (DPBS) to get a concentration of 1 x 1012 vector genomes/mouse in 100 µL.
- Place the viral solution into a 28-30 G needle on a 1 mL syringe. Be careful to avoid drawing air bubbles into the needle.
- Intravenous (i.v.) tail vein injection procedures
- Turn on the oxygen up to 0.5 L/min and set the isoflurane anesthesia system to 4%-5%. Place the mouse in the induction chamber for ~2 min, until the animal is not responsive.
- Place the animal on a mouse tail illuminator restrainer (e.g., Braintree Scientific, Inc. (Braintree, MA)) and accommodate the animal lying on its side. Use isoflurane anesthesia to 2%-3% for maintenance.
NOTE: The heating by the restrainer device will cause dilation of the mice tail vein and, hence, make significantly easier to inject. - Identify the lateral tail vein. Clean the injection area with an antiseptic using a gauze pad.
- Hold the end of the tail to extend it, and massage the mouse tail with fingers until the vein is visualized. Insert the needle at a low angle (10-15-degree angle) and inject 100 µL of diluted AAV into the tail vein (Figure 2A).
- Withdraw the needle and apply pressure immediately with a finger until the bleeding stops. Return the mouse to the original cage.
2. P-407 preparation and administration
- P-407 preparation
- Prepare the solution by diluting the P-407 agent (see Table of Materials) with DPBS to a final concentration of 100 mg/mL inside a fume hood. Refrigerate the solution at 4 °C overnight on a rotator to facilitate the dissolving of the P-40710.
- Bi-weekly intraperitoneal (i.p.) injection procedure
- Weigh each mouse on the first day of i.p. injections. Using the formula 1 g/kg, calculate the appropriate dose for each mouse according to weights and prefill syringes.
- Under a fume hood, manually restrain the mouse with the head and body tilted downwards in order to reposition the internal organs cranially. This technique avoids puncture of vital structures in the vicinity.
- Identify the left peritoneal cavity in the lower quadrant of the abdomen, lateral to the midline. Clean the site with an antiseptic.
- At a 45-degree angle or less, insert the needle into the peritoneal cavity (Figure 2B). Aspirate the syringe to ensure adequate insertion.
- If blood or tissue is present on aspiration, withdraw the needle and repeat steps 2.2.2 -2.2.4 until the syringe is clear. Dispose of the needle in the appropriate sharps container and return the mouse to the original cage.
3. Echocardiography assessment
- Preparation
- Apply depilatory cream to the mouse's chest and upper abdomen the day before or several hours before imaging. Remove the cream with wet gauze after 2 min.
- Anesthetize the mouse with 2.5%-3.0% isoflurane at 0.8 L/min flow rate and maintain with 1%-1.5% isoflurane. Then, secure the mouse to the appropriate platform in the supine position with the paws on electrode pads with conducting gel and cover the nose and mouth with a nose cone to ensure continuous anesthesia with isoflurane.
- Parasternal long-axis view
- With the mouse positioned supinely, tilt the right side of the platform 45 degrees.
- Next, diagonally align the transducer probe in the rail system, angling it 30-40 degrees in a clockwise manner from the right upper extremity to the left abdomen to obtain and store B-mode images.
- Analyze the B-mode images using ultrasound analysis software (see Table of Materials) to obtain the ejection fraction (Figure 3A).
- Parasternal short-axis view
- Rotate the transducer probe in the rail system 90 degrees clockwise to obtain and store B-mode and M-mode images.
- Apical view
- Tilt the left upper corner of the platform downwards and towards the right. Orient the transducer towards the right shoulder of the animal.
- Visualize the mitral valve in B-mode and color Doppler mode. Acquire and store pulsed wave (PW) Doppler and tissue Doppler images5.
- Analyze the PW Doppler and tissue Doppler images using the ultrasound analysis software to obtain the IVRT, E/E', and E/A (Figure 3B-E).
4. Pressure-volume (PV) loop data recording
- Perform hemodynamic analyses at the conclusion of the study to assess left ventricle (LV) systolic and diastolic function, following the previously described procedure11,12.
- Begin by inducing the mouse with isoflurane (3-5%, induction chamber).
- When anesthetic action starts, transfer the animal to the surgical bench, and maintain anesthesia with isoflurane (1-3%, facemask).
- Make a small incision in the skin over the neck to permit endotracheal intubation (through the mouth).
- Ventilate the animal with a mixture of oxygen and isoflurane using a rodent ventilator (e.g., Micro vent model 848, Harvard Apparatus) set at ~0.15-0.2 mL volume and the respiratory rate at 120-170 breaths/min.
- Monitor body temperature at ~37 °C ± 1 °C throughout the procedure using a temperature controlled surgical table.
- Expose and cannulate the left internal jugular vein with a 30 G needle for fluid support administration.
- Cut the skin over the site of the median ventral neck and expose the carotid artery. After occlusion of the distal portion of the right carotid artery, make a small cut in the artery to permit the introduction of a micro-tipped pressure-volume (PV) catheter (see Table of Materials) into the left ventricle (closed chest approach).
- Record PV loops during steady state and inferior vena cava occlusion.
- At the end of the experiment, humanely euthanize the animal (under deep anesthesia) using an approved AVMA method (e.g., Isoflurane followed by cervical dislocation).
- Analyze the PV data using LabChart software (see Table of Materials), and calibrate volumes using echocardiographic measurements.
Representative Results
After 4 weeks of combined single dose i.v. AAV9-cTnT-LDLR and bi-weekly i.p. P-407 injections, echocardiography revealed HFpEF, as evidenced by the preserved ejection fraction, prolonged intraventricular relaxation time (IVRT) and E/E' as well as decreased E/A (Figure 3A-E). Worse diastolic dysfunction was observed after 8 weeks when compared with data after 4 weeks. Pressure-volume (PV) loop analysis after 8 weeks of treatment showed an increased end-diastolic pressure-volume relationship slope, corroborating the echocardiography findings of diastolic dysfunction (Figure 3F). Notably, sudden death occurred in a significant number of mice treated with LDLR/P-407 between 6 and 12 weeks post-treatment with LDLR/P-407 (Figure 3G). These results indicate cardio-metabolic HFpEF, confirming the effectiveness of this protocol and experimental design. Hyperlipidemia was noted in mice treated with LDLR/P407 at 4 and 8 weeks, as evidenced by elevated total cholesterol, triglycerides, very-low-density lipoprotein (VLDL), low-density lipoprotein (LDL) cholesterol, and normal high-density lipoprotein cholesterol levels, corroborating our findings of hyperlipidemia (Figure 3H).
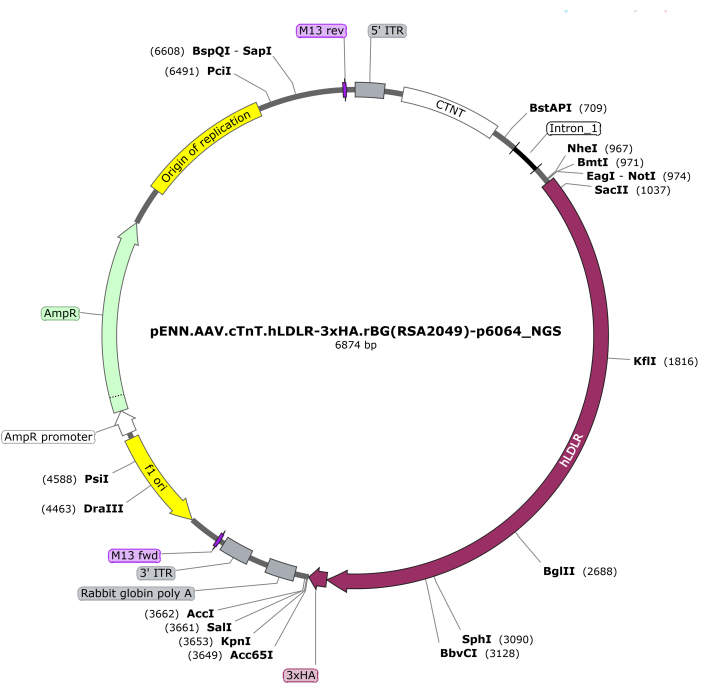
Figure 1: Plasmid map for AAV9-cTnT-LDLR. Please click here to view a larger version of this figure.
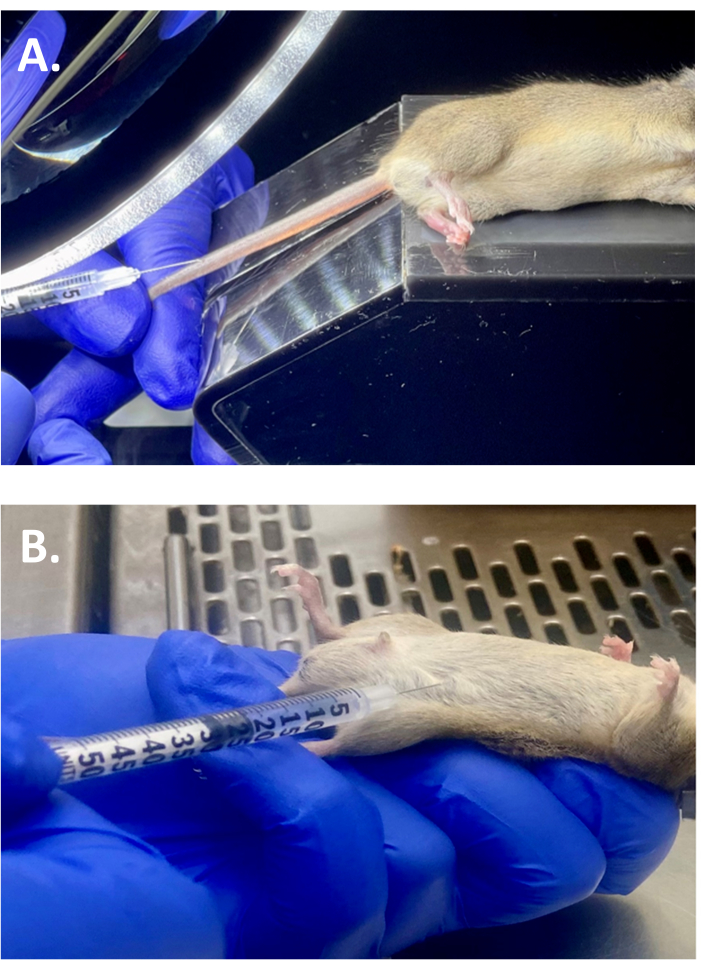
Figure 2: Injection procedures. (A) Representative image demonstrating the intravenous (i.v.) tail vein injection of AAV9-cTnT-LDLR in WT mouse on 129J strain background. (B) Illustration of intraperitoneal injection of P-407 in WT mouse on 129J strain background previously treated with single i.v. dose of AAV9-cTnT-LDLR. Please click here to view a larger version of this figure.
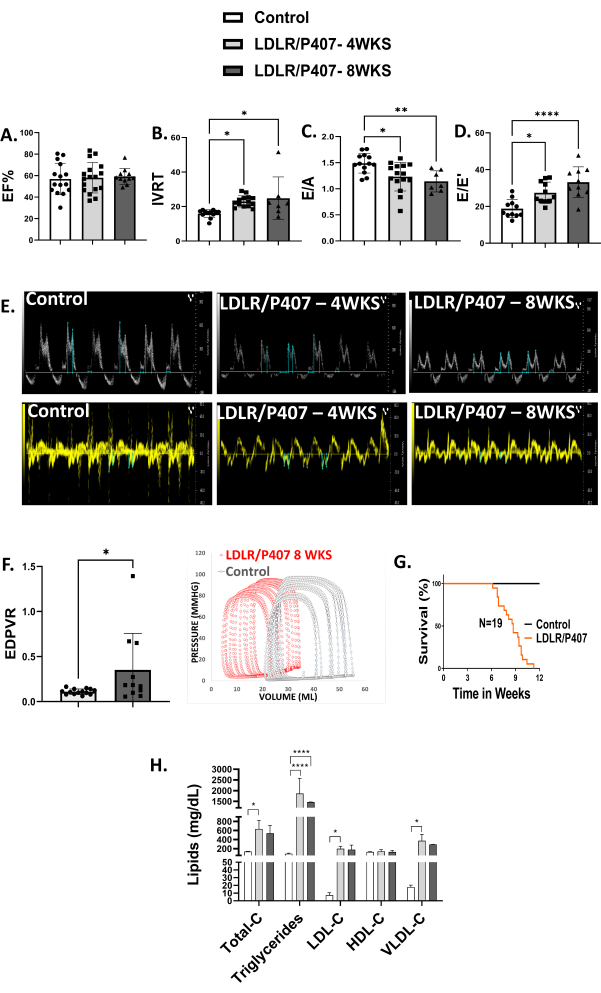
Figure 3: Cardio-metabolic HFpEF. (A–E) Echocardiography parameters indicating heart failure with preserved ejection fraction (HFpEF) after 4 (n = 17) and 8 weeks (n = 11) of LDLR/P-407 treatment compared to untreated mice (n = 15). This is evidenced by preserved ejection fraction, prolonged isovolumic relaxation time (IVRT), increased E/E' and reduced E/A, all indicators of diastolic dysfunction. (F) Pressure-volume loop acquisition and analyses revealed increased end-diastolic pressure-volume relationship (EDPVR) slope after 8 weeks of treatment. (G) Sudden death occurred between 6 and 12 weeks post-treatment with LDLR/P-407. (H) A lipid panel supported the findings of hyperlipidemia in mice treated with LDLR/P407 at 4 (n = 4) and 8 weeks (n = 3) as evidenced by elevated total cholesterol, triglycerides, very-low-density lipoprotein (VLDL), low-density lipoprotein (LDL) cholesterol, and normal high-density lipoprotein cholesterol levels compared to untreated mice (n = 5). The data is represented as mean ± SD. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001. Please click here to view a larger version of this figure.
Discussion
Despite the steady increase in the prevalence of HFpEF over the last decade, a concrete understanding of the underlying pathophysiology remains elusive13. Moreover, as of today, limited evidence-based therapy exists13. An improved understanding of the mechanisms involved in cardio-metabolic HFpEF is necessary. Previously, a hyperlipidemic mouse model was introduced that mimics HFpEF with neither chronic kidney disease (CKD) nor hypertension induced by cardiac LDLR OE and p407 injections9.
Findings revealed that the combination of cardiac LDLR OE and hyperlipidemia results in diastolic dysfunction, arrhythmias, left ventricular (LV) hypertrophy, exercise intolerance, cardiac lipid accumulation, and fibrosis in mice after four weeks, as previously published9. An increase in LDL-cholesterol uptake in the hearts, liver, and skeletal muscles and decreased triglycerides in the hearts and liver of these mice were also observed9. The advantage of this method lies in its rapidity for investigating the pathways of cardio-metabolic syndrome, which are not well understood compared to other hyperlipidemic HFpEF mouse models, such as the high-fat diet (HFD) that require up to 16 and 20 weeks to develop14. This model takes four weeks to develop and mimics metabolic abnormalities in humans. Therefore, the reproducibility of this model is essential.
It is imperative to ensure the thorough preparation and administration of AAV9-cTnT-LDLR and P-407. The replicability of this model is highly dependent on accurate calculations of P-407 and AAV9-cTnT- LDLR concentrations and doses, as well as weight measurements. Equally important are solution preparations and proper intravenous and intraperitoneal injection techniques. Deviations in these techniques may result in significant alterations and undesired results.
Despite the effectiveness and efficiency of this model, several limitations exist. Rigorous training is needed to perform intravenous and intraperitoneal injections. Additionally, there is a potential risk of morbidity and mortality associated with intravenous and frequent intraperitoneal injections. Mouse tail injuries may result when performing intravenous injections, while cecal puncture may occur with intraperitoneal injections, leading to peritonitis15. These injuries are typically due to incorrect techniques and may result in losing experimental subjects and treatment. Therefore, extensive training is necessary prior to performing these procedures. Another limitation is the focus of this model on the 129J strain. The rationale behind the choice of the 129J strain stems from preliminary studies that yielded more rapid diastolic dysfunction and HFpEF findings in this strain compared to the C57BL/6 mice we initially studied in unpublished investigations.
Regardless of these limitations, this model will allow for more rapid investigations into the underlying mechanisms involved in HFpEF and potential effective treatment options. Previous studies have led to the development of a pathophysiological model for cardiometabolic HFpEF-induced HFD and N[w]-nitro-l-arginine methyl ester (L-NAME) over 5-15 weeks13. However, due to the steady increase in the prevalence of HFpEF, there is an urgent need for further understanding of the pathophysiology of cardiometabolic HFpEF and the development of effective therapy. This murine model of cardiac LDLR OE and p407-induced hyperlipidemia is a rapid and feasible method of inducing cardiometabolic HFpEF for future research endeavors.
Declarações
The authors have nothing to disclose.
Acknowledgements
We thank the Penncore and NHLBI Gene Therapy Resource Program (GTRP) for funding the generation of the Adeno-associated virus used in this project. This research was funded by grants from the National Institute of Health (NIH) (1R01HL140468) and the Miami Heart Research Institute to LS. MW was a recipient of the NIH Diversity Supplement Award from 2020 – 2022 (R01HL140468- 03S1). JH is funded by 1R01 HL13735, 1R01 HL107110, 5UM1 HL113460, 1R01 HL134558, 5R01 CA136387 (from the NIH), W81XWH-19-PRMRPCTA (from the Department of Defense), and the Starr, Lipson, and Soffer Family Foundations.
Materials
| Adeno-associated virus 9-cardiac troponin T-LDLR (AAV9-cTnT-LDLR) | U. Penn Vector Core, funded by the NHLBI Gene Therapy Program (GTRP) | Transgene plasmids and AAVs particles were generated by the U. Penn Vector Core, funded by the NHLBI Gene Therapy Program (GTRP). AAV were provided in Dulbecco’s phosphate-buffered saline (PBS) with 0.001% Pluronic F68. The Core determined AAV titers by digital droplet polymerase chain reaction (ddPCR) and assessed all preparations for capsid protein ratio by SDS-PAGE and for the presence of endotoxin. Constructs include the human (h) transcripts tagged by 3X HA, Penn Vector Core (RRID: SCR_022432). AAV9-cTNT-hLDLR plasmid encodes the full human LDLR protein (2664bp). | |
| Imaging systems with a high frequency transducer probe MS400 | (VisualSonics, Toronto, ON, Canada) | Vevo 2100 or 3100 | |
| Isoflurane | Akorn Animal Health, Inc. | NDC: 59399-106-01 | |
| LabChart software | ADInstruments | Pro version 8.1.5 | |
| Poloxamer 407 | Sigma-Aldrich | 16758 | |
| PV catheter | Millar Instrument | PVR 1035 | |
| Ultrasound analysis software | Vevo Lab | ||
| Wild-type (WT) mice on 129J background | Jackson Laboratory |
Referências
- Roger, V. L. Epidemiology of heart failure: A contemporary perspective. Circ Res. 128 (10), 1421-1434 (2021).
- Kosiborod, M. N., et al. Design and baseline characteristics of step-HFpEF program evaluating semaglutide in patients with obesity hfpef phenotype. JACC Heart Fail. 11 (8), 1000-1010 (2023).
- Borlaug, B. A. Evaluation and management of heart failure with preserved ejection fraction. Nat Rev Cardiol. 17 (9), 559-573 (2020).
- Badrov, M. B., Mak, S., Floras, J. S. Cardiovascular autonomic disturbances in heart failure with preserved ejection fraction. Can J Cardiol. 37 (4), 609-620 (2021).
- Wu, C. K., et al. Myocardial adipose deposition and the development of heart failure with preserved ejection fraction. Eur J Heart Fail. 22 (3), 445-454 (2020).
- Hahn, V. S., et al. Myocardial gene expression signatures in human heart failure with preserved ejection fraction. Circulation. 143 (2), 120-134 (2021).
- Korolenko, T. A., et al. Early-stage atherosclerosis in poloxamer 407-induced hyperlipidemic mice: Pathological features and changes in the lipid composition of serum lipoprotein fractions and subfractions. Lipids Health Dis. 15, 16 (2016).
- Patel, M., et al. Osteopontin and ldlr are upregulated in hearts of sudden cardiac death victims with heart failure with preserved ejection fraction and diabetes mellitus. Front Cardiovasc Med. 7, 610282 (2020).
- Williams, M., et al. Mouse model of heart failure with preserved ejection fraction driven by hyperlipidemia and enhanced cardiac low-density lipoprotein receptor expression. J Am Heart Assoc. 11 (17), e027216 (2022).
- Colly, A., Marquette, C., Courtial, E. J. Poloxamer/poly(ethylene glycol) self-healing hydrogel for high-precision freeform reversible embedding of suspended hydrogel. Langmuir. 37 (14), 4154-4162 (2021).
- Kanashiro-Takeuchi, R. M., et al. Efficacy of a growth hormone-releasing hormone agonist in a murine model of cardiometabolic heart failure with preserved ejection fraction. Am J Physiol Heart Circ Physiol. 324 (6), H739-H750 (2023).
- Dulce, R. A., et al. Synthetic growth hormone-releasing hormone agonist ameliorates the myocardial pathophysiology characteristic of heart failure with preserved ejection fraction. Cardiovasc Res. 118 (18), 3586-3601 (2023).
- Borlaug, B. A., et al. Obesity and heart failure with preserved ejection fraction: New insights and pathophysiological targets. Cardiovasc Res. 118 (18), 3434-3450 (2023).
- Noll, N. A., Lal, H., Merryman, W. D. Mouse models of heart failure with preserved or reduced ejection fraction. Am J Pathol. 190 (8), 1596-1608 (2020).
- Guarnieri, M. Considering the risks and safety of intraperitoneal injections. Lab Anim (NY). 45 (4), 131 (2016).
