Eleven formalin-fixed cadavers were included, with an average age of 80.5 years6. Two cadavers had damaged lumbar vertebrae on the right side and were removed. Thus, a total of 20 measurements were included, 13 female and 7 male. The medial border of the safe zone, defined by the most lateral aspect of the lumbar plexus, was found to be approximately 1 cm medial to the tip of the TP at L1–L3, but narrowed down to approximately 6 and 1 mm at L4 and L5, respectively. The medial border of the safe zone was then subtracted by the distances of the cranial and caudal tip of each TP to the lateral edge of the psoas muscle at each level. This calculation gave us the medial to lateral area of safe debridement. The average area of the safe zone for debridement, at all levels of the lumbar spine, was found to be between 4 and 8 mm.
The area for maximum medial to lateral irrigation and debridement in the coronal plane was determined by measuring the distance from the superior and inferior tips of the TP to the lateral edge of the psoas muscle at the corresponding vertebral level. On average, the maximal extent of lateral debridement one can perform is as follows: 5.5 and 5.7 mm medial to the inferior and superior tips of the TP at L1, 4.7 and 5.1 mm medial at L2, 1.8 and 2.5 mm medial at L3, 0 and 0.4 mm medial at L4, and 3.8 and 3.7 mm lateral at L5. In the sagittal plane, the lumbar plexus was approximately 15–20 mm anterior to the TP. (Table 1).
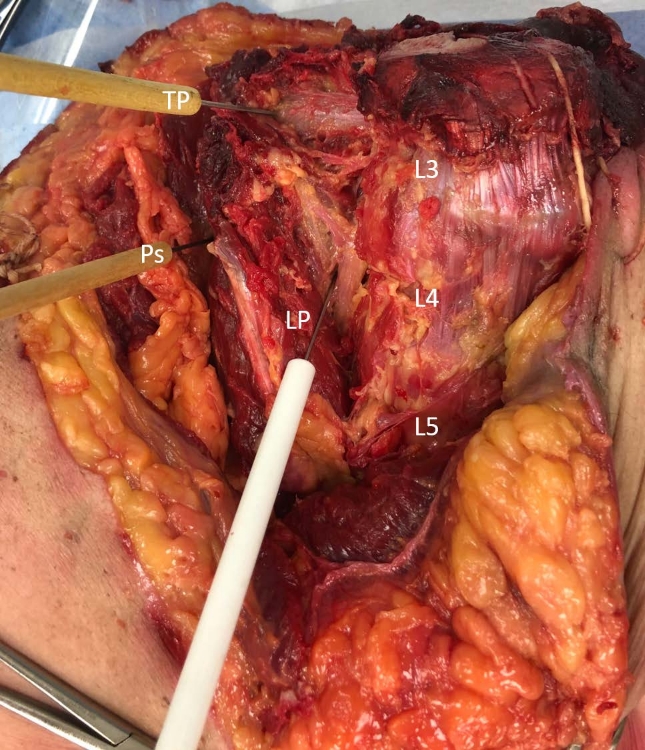
Figure 1: Cadaveric image of an anterior approach dissection. The TP, LP and psoas are clearly defined and used as the reference points for measurements. TP = transverse process; LP = lumbar plexus; Ps = lateral edge of psoas; L3, L4, L5 = lumbar vertebrae. Please click here to view a larger version of this figure.
| Lumbar Vertebra | ||||||
| Measurement | L1 | L2 | L3 | L4 | L5 | |
| Lateral superior tip of TP to lateral edge of psoas | -5.7 ± 1.92 | -5.11 ± 1.84 | -2.52 ± 2.63 | -0.42 ± 2.39 | 3.70 ± 1.60 | |
| Lateral inferior tip of TP to lateral edge of psoas | -5.49 ± 2.02 | -4.70 ± 1.71 | -1.84 ± 2.56 | -0.03 ± 2.31 | 3.77 ± 1.57 | |
| Lateral superior tip of TP to lateral edge of LP | -9.3 ± 1.94 | -11.75 ± 1.59 | -10.47 ± 2.90 | -6.64 ± 2.53 | -1.01 ± 2.31 | |
| Lateral inperior tip of TP to lateral edge of LP | -9.2 ± 2.06 | -11.71 ± 1.54 | -9.8 ± 2.47 | 6.24 ± 2.43 | -0.89 ± 2.40 | |
| Lateral edge of LP to lateral edge of psoas calculated using the lateral superior tip of the TP | 3.96 ± 0.98 | 6.64 ± 1.17 | 7.94 ± 2.00 | 6.22 ±1.28 | 4.71 ± 1.38 | |
| Lateral edge of LP to lateral edge of psoas calculated using the lateral inferior tip of the TP | 4.03 ± 1.05 | 7.0 ± 1.15 | 7.96 ± 2.00 | 6.21 ± 1.77 | 4.66 ± 1.59 | |
| Lateral superior tip of the TP to the LP in the saggital plane | 17.89 ± 2.72 | 19.08 ± 1.93 | 19.50 ± 3.12 | 16.26 ± 2.69 | 14.97 ± 1.90 | |
| Lateral inferior tip of the TP to the LP in the saggital plane | 17.84 ± 3.03 | 18.65 ± 1.60 | 19.19 ± 3.06 | 16.27 ± 2.93 | 14.92 ± 1.85 | |
Table 1: Mean value in millimeters of 20 sets of measurements, 13 female and 7 male. Negative values indicate that the measurement is medial to the tip of the TP. The distance of the lateral edge of the psoas to the most lateral region of the LP defines the safe zone for medial to lateral debridement. The distance from the tip of the TP to the LP in the sagittal plane defines the safe zone for debridement in the sagittal plane.
