Table 2 presents the median anatomical parameters for the major cardiac veins for 42 human heart specimens. All heart specimens contained one posterior interventricular vein (PIV) and anterior interventricular vein (AIV). Some specimens contained more than one posterior vein of the LV (PVLV), postero-lateral vein (PLV), left lateral vein (LLV), and/or antero-lateral vein (ALV), while other hearts may not have had one or two of these specific veins present.
| Materials Used |
| Perfusion-fixed Human Hearts |
| Venogram Balloon Catheters |
| Polymer Sealable Container |
| Anatomically correct heart sponge |
| CT scanner and software |
| Contrast and Saline Injector |
| Contrast (omnipaque) |
| Mimics Software |
Table 1. Summary of the materials used in the presented methodology.
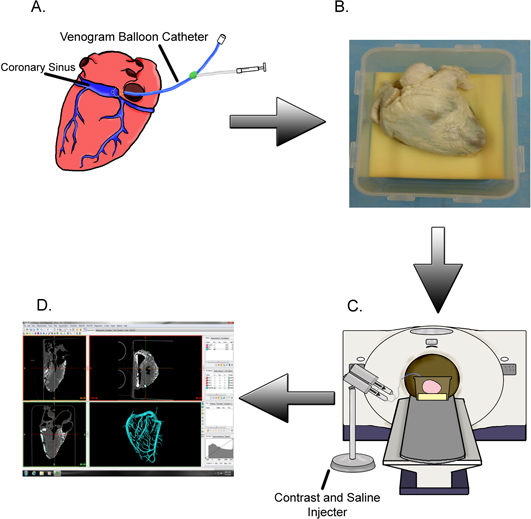
Figure 1. Methods summary. (A) The coronary sinus of a given isolated perfusion-fixed heart is cannulated with a venogram balloon catheter and (B) placed in its attitudinally correct position. (C) The specimen is scanned while contrast is injected into the cardiac venous system followed by a saline flush. (D) The generated images are used to create digital reconstructions of the veins so that subsequent measurements may be taken.
Video 1. An example of a 3D cardiac venous model generated from contrast-computed CT. Click here to view video.
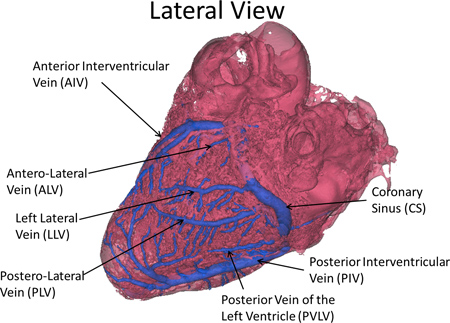
Figure 2. Nomenclature of the major vessels of the cardiac venous system.

Table 2. Summary of the measurements obtained to date for 42 human heart specimens. Click here to view larger table.
