In vivo monitoring of intestinal wound healing
During routine endoscopy, mucosal wounds were induced mechanically by miniature biopsy forceps with a diameter of 3 French (equals 1 mm; Figure 1A). Subsequently, wound healing was monitored by daily endoscopic examinations and quantified by measurement of the residual wound area using image editing software, e.g., ImageJ (Figure 1B). The individual wound closure over time is expressed by the quotient of actual wound area / initial wound area. For example, at day 3 after wound generation, 41% ± 4.1% of the wound area was recovered, whereas at day 7 the wound was usually completely healed (Figure 1C). Additionally, at the end of the experiment, wounds can be resected for histological evaluation ex vivo. Depicted are representative images of hematoxylin and eosin (H&E)-stained wound beds at day 0 and day 5 (Figure 1D).
Endoscopy-guided intramucosal injection therapy
For intramucosal application of pharmacological agents, a flexible tube (diameter of 0.96 mm) with a cannula fixed to the end (30 G) was introduced to the working channel of the endoscope (Figure 2A). After intramucosal placement of the needle, a maximum of 50 µl was carefully injected. Indicative of successful intramucosal application, lifting of the colonic mucosa can be easily observed macroscopically (Figure 2B,C).
In vivo assessment of experimental colitis
After induction of colitis, mice showed weight loss from day 3 with maximum loss of body weight of 19% occurring at day 7 (Figure 3A). In addition to daily measurement of body weight, disease activity was monitored by repetitive endoscopies and macroscopic quantification of inflammation by the murine endoscopic index of colitis severity (MEICS). In accordance with the loss of body weight, MEICS score was increased at day 7 after DSS start indicating a massive inflammatory damage of the colonic mucosa, which was ameliorated at day 13 (Figure 3B). For ex vivo correlation of histological damage, inflammatory alterations of colonic H&E-stained sections were quantified according to the Dieleman Score 11. At day 7 after DSS start, histological damage was significantly higher in DSS-treated mice compared to controls as reflected by epithelial denudation, mucosal ulcerations as well as increased neutrophil infiltration and was significantly improved at day 13 (Figure 3C, E). In addition, histological evaluation of mucosal biopsies, routinely obtained during endoscopic examinations, corroborated the advanced stage of colitis at day 7 (Figure 3F-H).
Fluorescence endoscopy of colorectal tumors
Approximately 80 days after tumor induction by AOM and three cycles of DSS (Figure 4A), multiple colonic tumors (Figure 4C) as well as macroscopic signs of chronic inflammation such as granulated mucosa (Figure 4B) 10 were observed endoscopically. Histological evaluation of colorectal tumors by H&E staining revealed adenomas with and without high-grade intraepithelial neoplasia. Therefore, the AOM-DSS-model resembles a perfect model to study molecular processes of carcinogenesis 12, as well as to evaluate new diagnostic devices13. Fluorescence imaging targeting specific molecules allows in vivo molecular imaging with ‘photographic methods’ 14,15. To demonstrate feasibility of FE, we used FITC, a widely used fluorochrome. For specific FITC detection, a bandpass filter system combined with the light source provided specific excitation wavelength needed (490 nm; Figure 4D). For accurate detection of FITC-specific emission wavelength (525 nm), a second bandpass filter was interposed between the camera head and the endoscope (Figure 4E). FE without tracer application did not detect any specific signal and no interaction with colonic tissue or fecal autofluorescence (Figure 4F, G). In contrast, immediately after intravenous application of FITC-dextran, the fluorochrome could be observed at the colonic mucosa and may be used for assessment of increased vascularity in regions of chronic inflammation (Figure 4H) as well as malignant mucosa (Figure 4I). Accordingly, quantification of fluorescence intensity by an image editing software showed significantly increased uptake of the fluorochrome within malignant tissue as compared to non-affected colonic mucosa (Figure 4K).

Figure 1. Endoscopic monitoring of epithelial wound healing in vivo as well as quantitative and histological assessment of wound healing. After generation of colonic wounds, wound border and wound closure can be easily detected. The wound area (white arrows) is assessed during daily follow-up endoscopies to quantitatively follow epithelial wound healing (A–C). Ex vivo, wounds were resected and H&E-stained for histological analysis of wound healing (D). Scales are defined by depicted scale bar. Please click here to view a larger version of this figure.
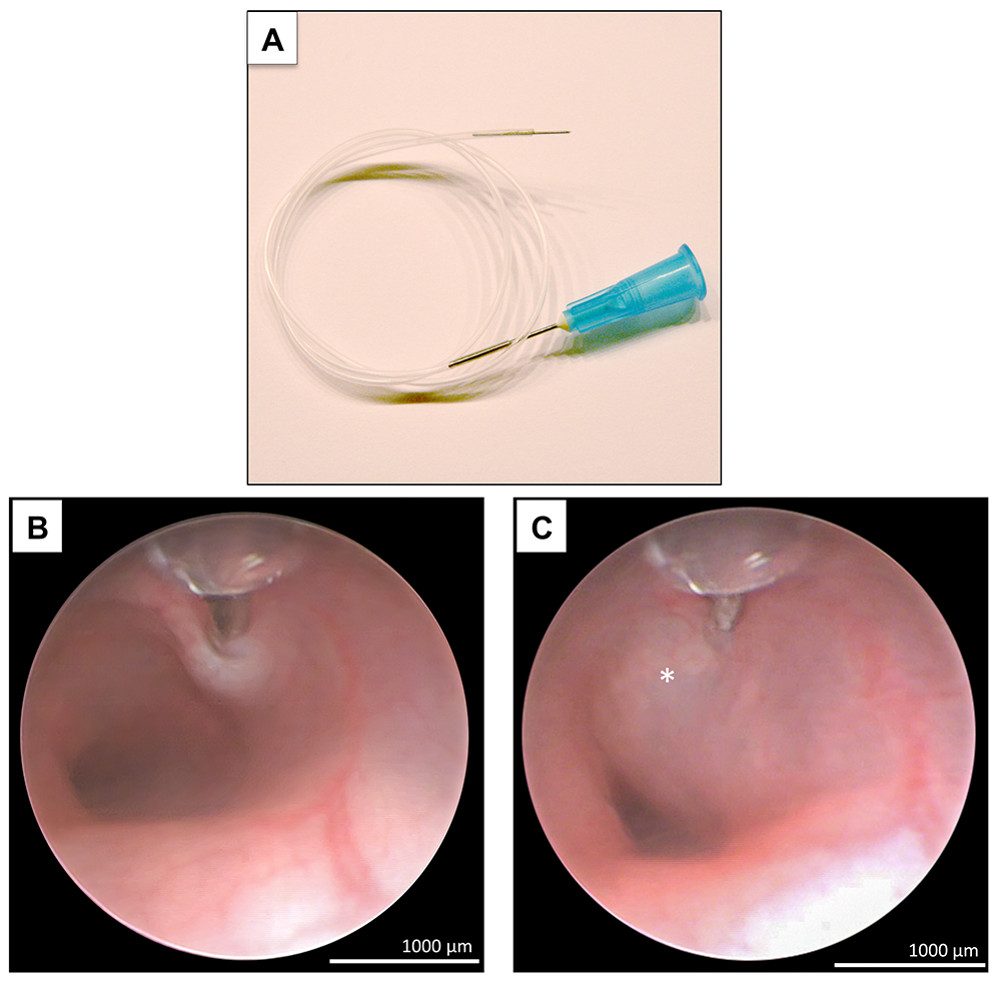
Figure 2. Endoscopy-guided intramucosal injection therapy. Under visual control, the tip of the needle (A) is softly placed into the colonic mucosa and 50 µl of dissolved substances is injected (B). Subsequently, marked mucosal lifting can be recognized (asterisk) without any signs of acute bleeding (C). Scales are defined by depicted scale bar. Please click here to view a larger version of this figure.

Figure 3. Endoscopic evaluation of the course of experimental DSS colitis. The course of colitis was evaluated by changes in body weight, endoscopic examinations as well as histological analysis of inflamed colonic sections and endoscopic biopsies. In line with massive loss of body weight and advanced histological damage at day 7 (A, C, E; magnification 10X), endoscopic examinations and histological evaluation of obtained biopsies depicted signs of severe inflammation (B, D, G, H; magnification 5X and 10X) whereas at day 13 after DSS start inflammatory alterations were significantly ameliorated. Scales are defined by depicted scale bar. Please click here to view a larger version of this figure.

Figure 4. FE of colorectal tumors. After induction of colorectal cancerogenesis by AOM and cyclic DSS administration for 11 weeks (A), white light endoscopy detected granulated mucosa indicative of chronic colitis (B) and numerous endoluminal lesions (C) which were diagnosed as adenomas with high-grade intraepithelial neoplasia by H&E staining ex vivo (G). While visualization of chronic inflammation (H) and tumors (I) was easily possible using FE targeted FITC, FE without tracer application did not allow definitive tumor detection (F, G). Accordingly, quantification of fluorescence intensity was significantly increased within malignant tissue as compared to non-affected colonic mucosa, shown by gray scale profiles (E, F). To switch to the fluorescence mode during white light colonoscopy, a specific bandpass filter is additionally plugged into the cold-light source to provide the specific excitation wavelength (e.g., 490 nm for FITC; D). This filter facilitates switching (white arrow) between white light and fluorescence modes (D). To capture the specific emission wavelength (e.g., 525 nm for FITC), a second bandpass filter is interposed between endoscope and camera head using a bayonet joint (E). Scales are defined by depicted scale bar. Please click here to view a larger version of this figure.
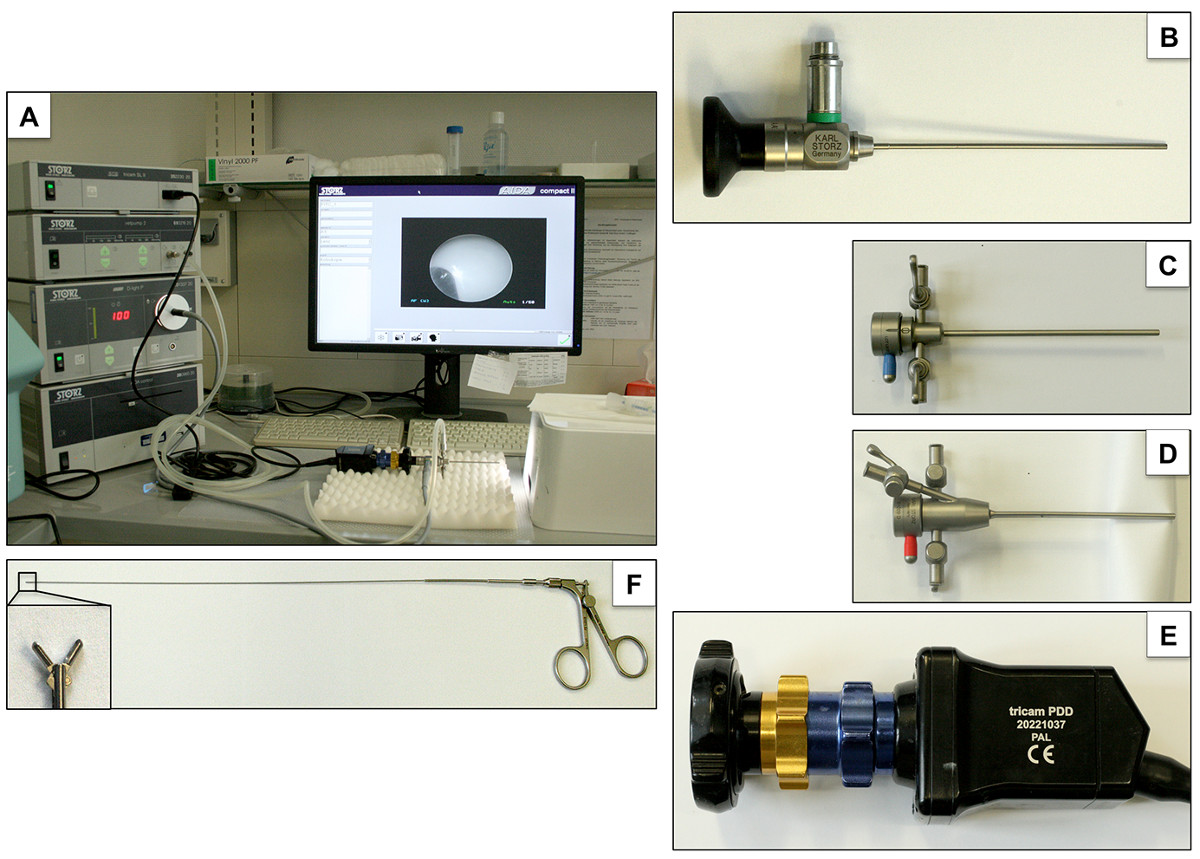
Figure 5. Experimental set-up of endoscopic working station. The endoscopic working station (A) consists of the following components: straightforward telescope (0°, diameter: 1.9 mm, length: 10 cm; B), endoscope sheath (9 Charr.) without (C) and with working channel (D), camera (E) and biopsy forceps (F). Please click here to view a larger version of this figure.
