When looking at Figure 1, it is clear that the quadricep of the rabbit is enlarged. Additionally, multiple small discrete nodules, typically correlating with tumor growth through the fascia, are visible. Upon palpation, the injected limb should appear than the non-injected limb. If a researcher requires more definitive assurance of tumor presence, ultrasound imaging can be used to identify the tumor embedded in the muscle. If a tumor is not detected, the hind limb should be re-injected with a tumor cell suspension.
In order to confirm successful vascular access, blood return into the sheath is observed on aspiration as seen in Figure 13D. If vascular access was unsuccessful, attempted aspiration will yield air in the sheath or present with significant resistance when pulling the plunger of the syringe.
For liver tumor growth, there are two ways to confirm successful propagation: angiographically and on necropsy. On angiography, identification of the tumor may occur immediately as is the case in Figure 14A where the tumor draws blood supply directly from the common hepatic artery. It may also take some time in cases where the tumor is lateral as is the case in Figure 14D. If the tumor is not readily visible after injection of contrast into the common hepatic artery, the researcher should attempt to inject contrast into left and right hepatic arteries in order to improve the chances of highlighting the tumor. It may also help to look for aberrant arteries traveling laterally towards the distal edge of the liver as seen in Figure 14C. On necropsy, the tumor should be readily visible as seen in Figure 15B (compare to Figure 15A).
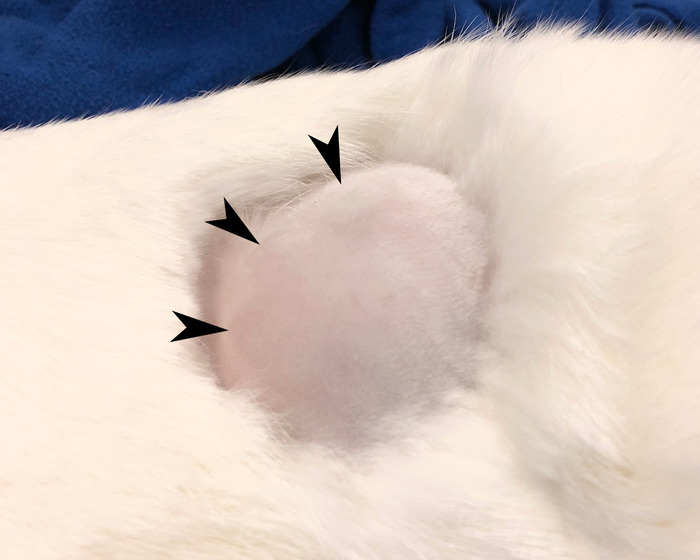
Figure 1: Rabbit hind limb. Shaved rabbit hind limb with mass indicative of tumor growth. Please click here to view a larger version of this figure.

Figure 2: Exposed hind limb. The same limb as shown Figure1 with overlying skin reflected revealing a large area of hypervascularity and discoloration distinct from the surrounding muscle representing the location of the tumor (white dotted line). Please click here to view a larger version of this figure.
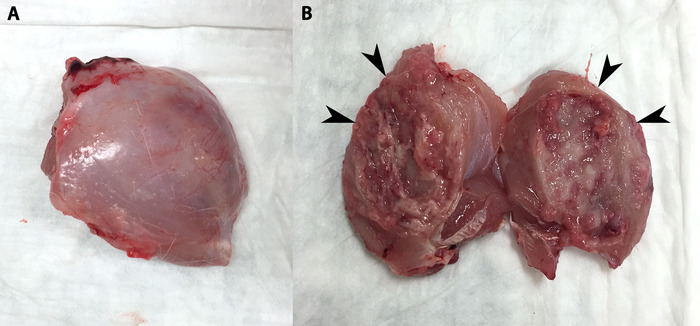
Figure 3: Tumor removed en bloc and bisected. (A) Tumor and surrounding muscle removed en bloc. (B) Tumor has been bisected to reveal its capsular wall (arrowheads) and necrotic core. Tumor process can be seen in both halves as well as some necrotic debris. Please click here to view a larger version of this figure.
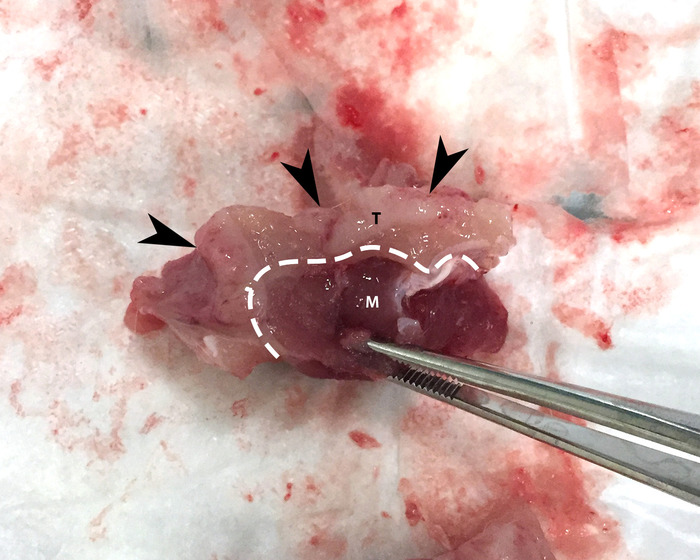
Figure 4: Tumor capsule. Arrowheads denote a piece of tumor (T), which is delineated from adjacent muscle (M) by the tumor capsule (dashed white line). Please click here to view a larger version of this figure.
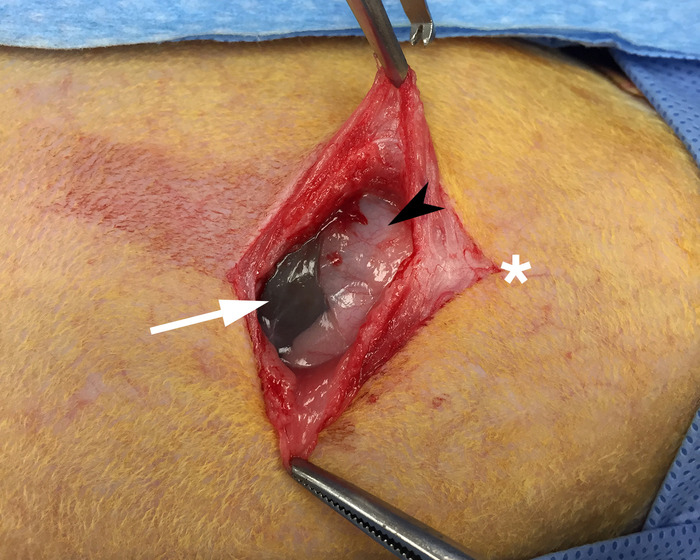
Figure 5: Exposed xiphoid process. Skin and underlying muscle have been reflected to allow for visualization of the xiphoid process (black arrow) and gut (white arrow). The white star denotes the cranial direction. Please click here to view a larger version of this figure.
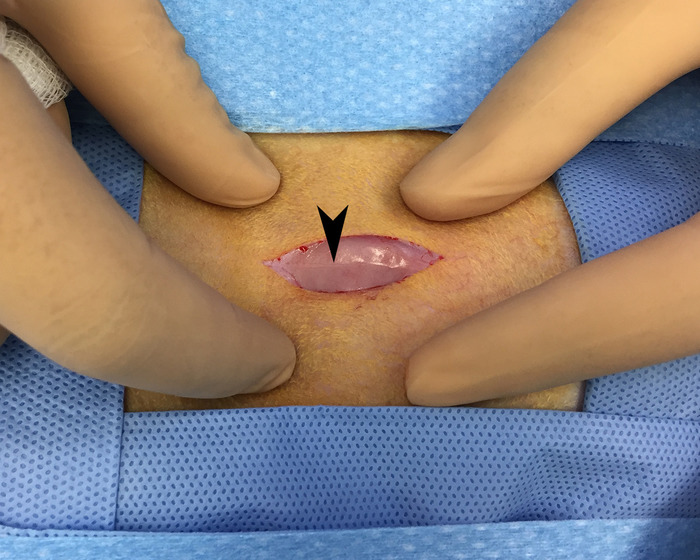
Figure 6: Linea alba. Overlying skin and fascia have been reflected to allow for visualization of the linea alba (black arrow) running in a cranial to caudal direction. This area is avascular and provides for blood-loss free access of the peritoneal space. Please click here to view a larger version of this figure.

Figure 7: Lobe of liver outside peritoneum. This image shows a lobe of the liver that was gently extracted from the peritoneal space and placed on a piece of gauze. Please click here to view a larger version of this figure.
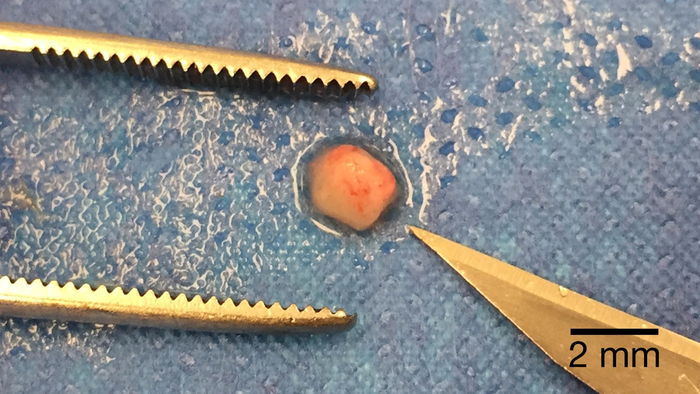
Figure 8: Post-processed tumor piece for implantation. A piece of tumor processed to the appropriate size for implantation placed next to the tip of a #11-blade for scale. Please click here to view a larger version of this figure.
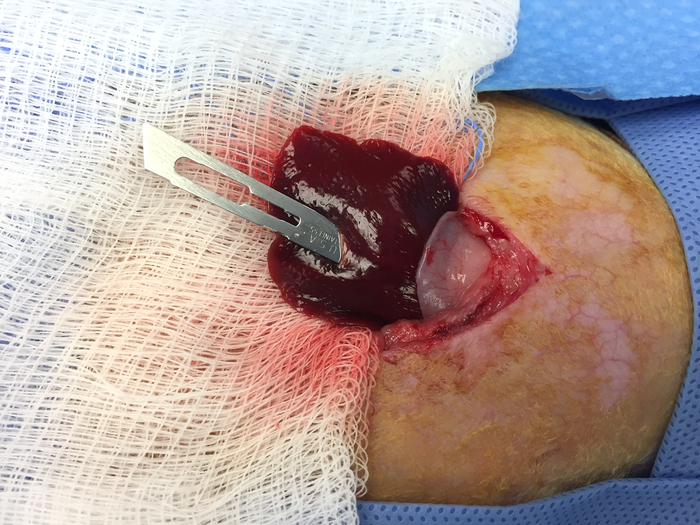
Figure 9: Creating a pocket in the liver for tumor implantation. An #11-blade is inserted to the appropriate depth in the extracted lobe of the liver. This will create an appropriately sized pocked for the implantation of the tumor piece from Figure 8. Please click here to view a larger version of this figure.
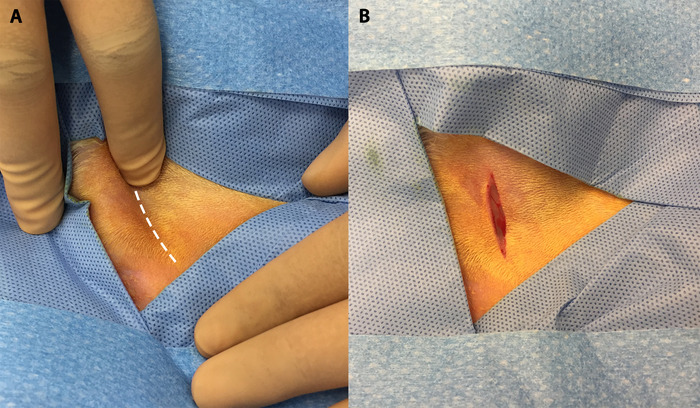
Figure 10: The femoral groove and initial incision. (A) Palpation of the hind limb allows for visualization of the femoral groove (white dotted line). (B) Initial incision in the hind limb made along the femoral groove. Please click here to view a larger version of this figure.
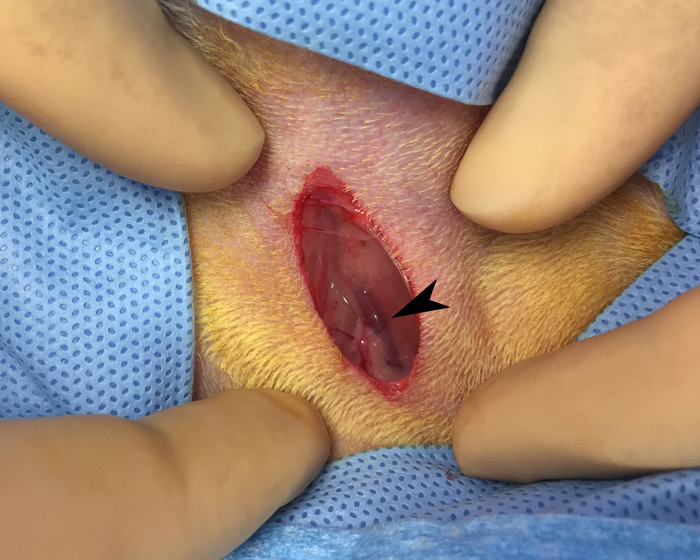
Figure 11: Identification of the femoral bundle. Blunt dissection of the initial incision reveals femoral vein (black arrow). Please click here to view a larger version of this figure.
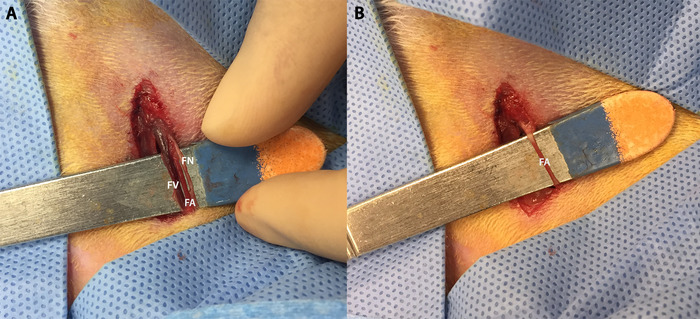
Figure 12: Dissection of femoral bundle and isolation of femoral artery. (A) Dissection of the femoral bundle allows us to individually distinguish (from left to right) the femoral vein (FV), femoral artery (FA), and femoral nerve (FN). (B) The femoral artery isolated on a scalpel handle. Note the blood column allowing for distinction from the femoral nerve. Please click here to view a larger version of this figure.
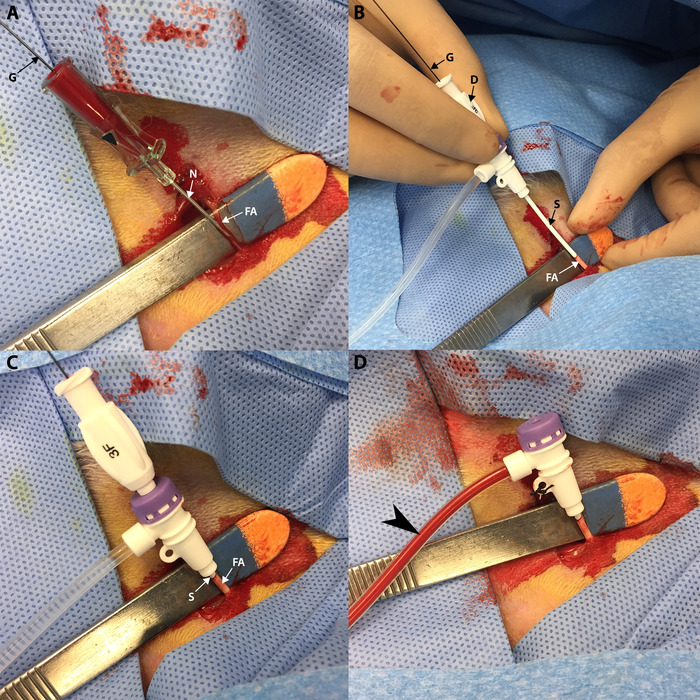
Figure 13: Vascular access. (A) A guidewire (G) is advanced into the femoral artery (FA) through the access needle (N) which was previously inserted into the femoral artery. (B) A sheath (S) and dilator (D) are advanced over the guidewire (G) into the femoral artery (FA). (C) Sheath (S) and dilator are advanced fully into the femoral artery (FA) up to the sheath hub. (D) Sheath is secured with silk after the dilator and guidewire have been removed. Aspiration yields blood (black arrow) in the sheath. Please click here to view a larger version of this figure.
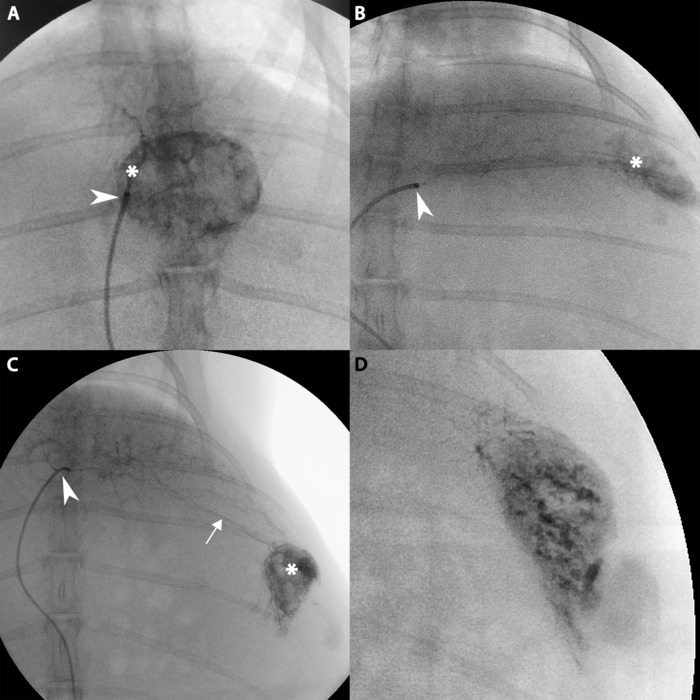
Figure 14: Angiographic imaging of hepatic tumor. (A) Catheter tip (white arrow) delivering contrast directly into artery feeding the tumor (white star). (B) Catheter tip (white arrow) delivering contrast into distal left hepatic artery and moderate contrast uptake by lateral tumor (white star). (C) Further contrast injection into tumor from B demonstrating an aberrant artery (white line) traveling from the catheter (white arrow) to the tumor (white star). (D) The tumor from B after further contrast uptake. Please click here to view a larger version of this figure.
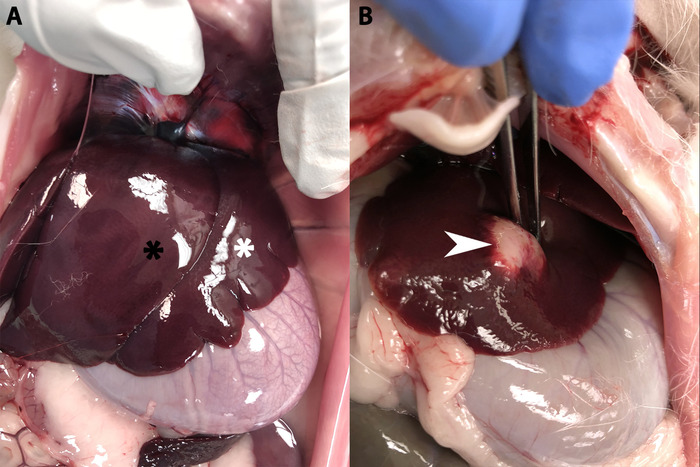
Figure 15: Rabbit liver. (A) A healthy rabbit liver showing the left medial lobe (white star) overlying the left lateral lobe (black star). (B) A rabbit liver with a fully developed hepatic tumor (white arrow). Please click here to view a larger version of this figure.
