The needle tip should be in the optimal area as shown in Figure 1. In selective CLS, the contrast is injected behind the anterior fascia of the psoas major muscle, targeting gray rami communicantes. A comparison of contrast spreading in selective CLS (A) and conventional CLS (B) is shown in Figure 2.
The expected clinical effects are vasodilation (for treatment of Raynaud's syndrome, livedo reticularis, thromboangiitis obliterans, ischemic diabetic foot, and erythromelalgia; Figure 3), sweat reduction (for treatment of hyperhidrosis), and pain relief (for treatment of erythromelalgia and phantom limb pain).
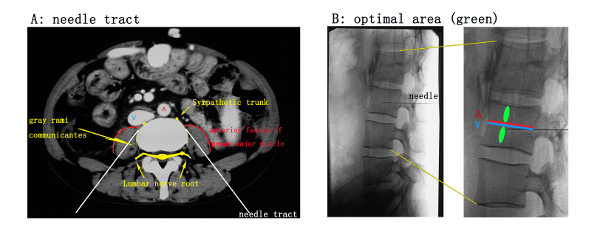
Figure 1: Relationship between puncture needle and surrounding organs/tissues. (A) A diagram of an axial lumber CT scan at the level of the needle tract. The white line represents the needle tract. It should be noted that the needle tip reaches close proximity to, but does not break through, the anterior fascia of the psoas muscle (red arc). A = abdominal aorta, V = inferior vena cava. (B) Lateral view of a lumbar X-ray. The green area illustrates the optimal area, located beside the lumbar vessels (usually located in the middle of the vertebral body horizontally), behind the anterior fascia of the psoas muscle and away from the lumbar nerve root behind the vertebral body. This is a safe location, closest to the gray rami communicantes. A = lumbar artery, V = lumbar vein. Please click here to view a larger version of this figure.
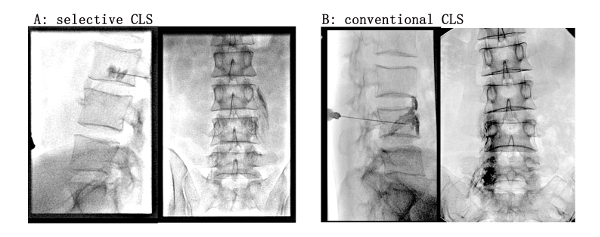
Figure 2: Comparison of contrast agent spreading in X-ray views between selective CLS (A) and conventional CLS (B). (A) Selective CLS. The contrast agent was injected behind the anterior fascia of the psoas muscle. The lateral view showed that the contrast agent spread around and behind the needle tip. The anterior-posterior (AP) view showed that the contrast agent diffused outward and downward along the spaces among psoas muscle fibers and formed thin strips, outlining the contour of the muscle fibers. (B) Conventional CLS. The contrast agent was injected in front of the anterior fascia of the psoas muscle. The lateral view showed that the contrast was concentrated in loose tissue in front of the needle tip. The AP view showed that the contrast agent was concentrated along the vertebral body, thus overlapping with the vertebral body in X ray view, and did not diffuse outward. Please click here to view a larger version of this figure.

Figure 3: Clinical observation after selective CLS on the right side of a patient with erythromelalgia. The patient's blood vessels dilated, skin temperature increased, and skin was rosy and dry on the right limb. In contrast, skin was damp and cold with a slight violaceous skin color on the left side without treatment. Please click here to view a larger version of this figure.
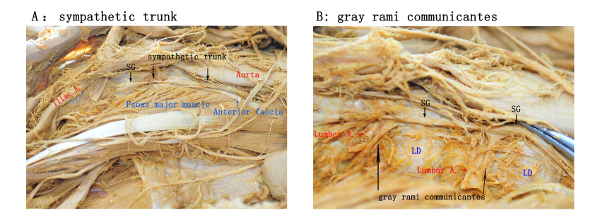
Figure 4: Anatomic illustration of sympathetic trunk and gray rami communicantes. (A) Anatomically, the psoas muscle is attached to the lateral side of the vertebral body and the lumbar disc (LD). In this illustration, most of the anterior fascia of the psoas muscle is removed, exposing the psoas muscle. The lumbar sympathetic trunk, located in front of the anterior fascia and adjacent to the abdominal aorta (right lumbar sympathetic trunk adjacent to inferior vena cava, not shown). The enlarged lumbar sympathetic ganglia (SG) are also visible. (B) With the psoas muscle removed from the outside of the vertebral body, the lumbar blood vessels and gray rami communicantes covered in the deep side of the psoas muscle are exposed. The gray rami communicantes originate from the sympathetic ganglia, extend through the anterior fascia, extend backward along the lateral edge of the vertebral body, surround the lumbar blood vessels, and finally join the lumbar nerve roots. Please click here to view a larger version of this figure.
