We recently reported that ischemic stroke induction in mice alters the immune cell composition of the lungs11. Specifically, transient cerebral ischemia increased percentages of alveolar macrophages, neutrophils, and CD11b+ DCs, while diminishing percentages of CD4+ T cells, CD8+ T cells, B cells, NK cells, and eosinophils in the pulmonary compartment. Moreover, cellular alteration corresponded to significantly diminished levels of multiple chemokines in the lungs. Described here is a method for the isolation and identification of different immune cell populations in the pulmonary compartment. Representative results shown here were from mice that had undergone tMCAO induction and a sham operation.
We identified 13 different populations of immune cells in the lungs (L1-L13) using 3 sets of antibody combinations with each set containing 5-7 antibodies (Figure 1). Dead cells were excluded using a LIVE/DEAD stain in each set. Antibodies and markers for distinguishing different immune cell types are listed in Table 1. Alveolar and interstitial macrophages, CD103+ DCs, CD11b+ DCs, and eosinophils were identified in Set 1 (Figure 1A,B). Proinflammatory monocytes and neutrophils were identified in Set 2 (Figure 1C). During inflammatory responses, monocytes migrate to the site of inflammation, where these cells differentiate into monocyte-derived antigen presenting cells (mo-APCs)14. Downregulation of Ly6C and CCR2 are characteristic of monocyte differentiation, which can be evaluated using Set 215. CD4+ T cells, CD8+ T cells, B cells, plasmacytoid DCs, NK cells, and NKT cells were identified using Set 3 (Figure 1D).
To determine the quality of our single cell isolation protocol, we compared the number of viable cells and CD45+ immune cells isolated using the manual method with the cells isolated using a commercially available tissue dissociator (see Table of Materials), which is often used to isolate cells from tissues16,17,18,19,20. In the latter protocol, lung lobes were transferred into a dissociator-specific tube (see Table of Materials) following injection of the dissociation buffer, and the tissue was digested using the 37C_m_LDK_1 program. The total number of viable cells, percentage of CD45+ cells, and the total number of CD45+ cells obtained were comparable between the two methods (Figure 2A-C). The percentage of cell death among CD45+ cells using both protocols was ~ 10% (Figure 2D). These results suggest that the protocol presented here allows cell recovery with high yield and quality without the aid of an automated tissue dissociator.
A commercially available multiplex assay coupled with flow cytometric analysis was used to determine the concentration of 13 chemokines using 25 µL of sample (Figure 3). Two different sizes of beads were first identified by FSC/SSC (Figure 3A). Each bead is coated with 6-7 primary antibodies, which could be distinguished by fluorescence intensity in the APC channel (Figure 3B). The level of chemokines in the sample is proportional to the fluorescence intensity in the PE channel, which could be determined by MFI (Figure 3C). By comparing the MFI value of each chemokine with the standard curve constructed with known concentrations of chemokine, the concentration in the sample (per mg of tissue) can be determined.
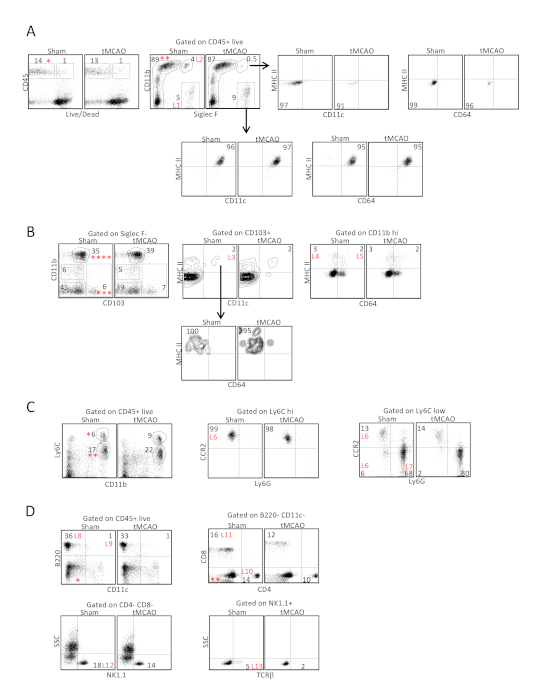
Figure 1: Identification of 13 immune cell types from the lungs following tissue digestion with collagenase D following ischemic stroke. Lung tissues were excised 24 h following tMCAO or sham operation, immune cells in the lungs were analyzed by flow cytometry, defined by surface markers listed on Table 1. (A) In antibody set 1, CD45+ viable cells (*) were first gated on Siglec F and CD11b to identify the alveolar macrophages (L1), which expressed CD11c and MHC II, and eosinophils (L2), which did not express CD11c and MHC II. (B) Cells within the Siglec F- population (**) in A were then gated to determine the expression of CD103 and CD11b. CD103+ CD11b- (***). Cells were further gated to determine the expression of CD11c and MHC II. CD103+ DCs expressed both CD11c and MHC II (L3) but did not express CD64. The CD11b hi population (****) was further gated to determine the expression of CD64 and MHC II. CD11b+ DCs expressed MHC II but not CD64 (L4), whereas interstitial macrophages (L5) expressed both markers. (C) In antibody set 2, CD45+ viable cells in A were gated to determine the expression of CD11b and Ly6C. Ly6C hi cells (*) represented the undifferentiated monocytes that maintained a high level of CCR2 expression (L6, middle plot), whereas Ly6C low cells (**) contained a mixed population of differentiating monocytes that were Ly6G- (L6, right plot), and Ly6G+ neutrophils (L7). (D) In antibody set 3, CD45+ viable cells in A were gated to determine the expression of CD11c and B220 to identify B cells (L8) and plasmacytoid DCs (L9). The CD11c- and B220- population (*) was then gated to determine the expression of CD4 and CD8 to identify CD4+ T cells (L10) and CD8+ T cells (L11). The CD4- CD8- population (**) was further gated to determine the expression of NK1.1 and TCRb to identify NK cells (L12) and NKT cells (L13). Shown are representative plots from 12 C57BL/6J mice following tMCAO and sham operation. Parts of the figure have been reprinted from previously published literature11 with permission. Please click here to view a larger version of this figure.
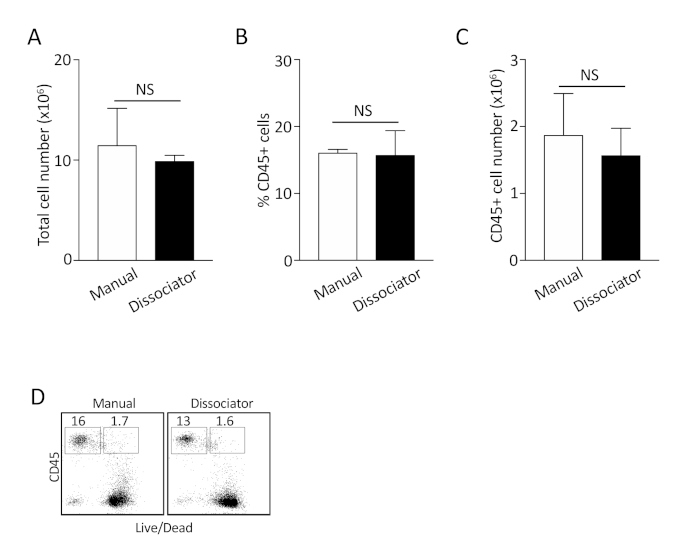
Figure 2: Comparison between manual dissociation method and the use of tissue dissociator for isolating single cells from the lungs. (A-C) The total number of cells, the percentage of CD45+ cells, and the total number of CD45+ cells were compared. Shown are combined results from 3 independent experiments. NS: not statistically significant. (D) Representative plots to determine the percentage of dead CD45+ cells following isolation. Shown are representative plots from 3 independent experiments. Please click here to view a larger version of this figure.
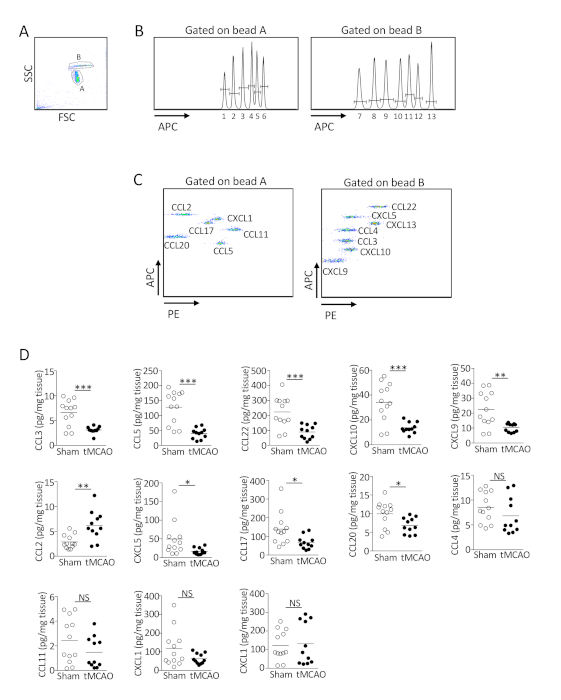
Figure 3: Ischemic stroke suppresses the production of multiple chemokines in the lungs. (A-C) Representative plots showing the determination of the level of 13 chemokines in the lungs by multiplex bead array. (A) FSC/SSC gate was used to identify beads A and B with different size. (B) Primary antibodies coated on the beads could be distinguished by fluorescence intensity in the APC channel. (C) The level of chemokines in the sample was proportional to the fluorescence intensity in the PE channel. Shown are representative plots from 12 C57BL/6J mice following sham operation. (D) Lung tissues were homogenized 24 h following tMCAO or sham operatio. The level of 13 chemokines in the lungs of individual animals was determined by multiplex bead array. Data shown are combined results from three independent experiments with n = 11-12 animals per group. *, P < 0.05; **, P < 0.01; ***, P < 0.001. NS, not statistically different. Parts of the figure have been reprinted from previously published literature11 with permission. Please click here to view a larger version of this figure.
| Antibody | Clone | Immune Cell Type | Population | Surface Marker Expression |
| CD45-FITC | 30-F11 | Alveloar macrophages | L1 | CD45+ Siglec F+ CD11b- |
| Siglec F-PE | E50-2440 | Eosinophils | L2 | CD45+ Siglec F+ CD11b+ |
| CD11c-Percp/Cy5.5 | N418 | CD103+ DCs | L3 | CD45+ Siglec F- CD11b- CD103+ CD11c+ MHC II+ |
| CD11b-PE/Cy7 | M1/70 | CD11b+ DCs | L4 | CD45+ Siglec F- CD11b hi CD103- CD64- MHC II+ |
| CD64-APC | X54-5/7.1 | Interstitial macrophages | L5 | CD45+ Siglec F- CD11b hi CD103- CD64+ MHC II+ |
| CD103-BV421 | 2E7 | |||
| MHC II-BV510 | M5/114.15.2 | |||
| Live/dead-APC/Cy7 | ||||
| CD45-FITC | 30-F11 | Monocytes/moDCs | L8 | CD45+ CD11b hi Ly6C hi/int CCR2+/- Ly6G- |
| Ly6C-PE | HK1.4 | Neutrophils | L9 | CD45+ CD11b hi Ly6C int CCR2- Ly6G+ |
| CD11b-PE/Cy7 | M1/70 | |||
| CCR2-BV421 | SA203G11 | |||
| Ly6G-BV510 | 1A8 | |||
| Live/dead-APC/Cy7 | ||||
| CD45-FITC | 30-F11 | Plasmacytoid DCs | L6 | CD45+ B220+ CD11c+ |
| CD8-PE | 53-6.7 | B cells | L7 | CD45+ B220+ CD11c- |
| NK1.1-Percp/Cy5.5 | PK136 | CD4+ T cells | L10 | CD45+ B220- CD11c- CD4+ CD8- |
| CD11c-PE/Cy7 | N418 | CD8+ T cells | L11 | CD45+ B220- CD11c- CD4- CD8+ |
| APC-B220 | RA3-6B2 | NK cells | L12 | CD45+ B220- CD11c- CD4- CD8- NK1.1+ TCRb- |
| CD4-BV421 | GK1.5 | NKT cells | L13 | CD45+ B220- CD11c- CD4- CD8- NK1.1+ TCRb+ |
| TCRb-BV510 | H57-597 | |||
| Live/dead-APC/Cy7 |
Table 1: Surface markers and antibody combinations for determining immune cells isolated from the lungs following tMCAO.
