صدمة القلب (CS) هي حالة نقص التروية في الأنسجة مع أو بدون انخفاض ضغط الدم المصاحب ، حيث لا يستطيع القلب تقديم ما يكفي من الدم والأوكسجين لتلبية متطلبات الجسم ، مما يؤدي إلى فشل الأعضاء. وتصنفه جمعية تصوير الأوعية الدموية القلبية الوعائية والتدخلات (SCAI): المرحلة A – المرضى المعرضين لخطر الإصابة ب CS؛ المرحلة A- 2000- 2003. المرحلة B – المرضى في المرحلة الأولى من CS مع انخفاض ضغط الدم أو عدم دقات القلب دون نقص التروية. المرحلة C – CS الكلاسيكية مع النمط الظاهري الباردة والرطبة التي تتطلب inotropes / فاسوبريسورس أو الدعم الميكانيكي للحفاظ على التغلغل؛ المرحلة D – تدهور الدعم الطبي أو الميكانيكي الحالي الذي يتطلب تصعيدا للأجهزة الأكثر تقدما؛ والمرحلة E – تشمل المرضى الذين يعانون من انهيار الدورة الدموية وعدم انتظام ضربات القلب الحراري الذين يعانون بنشاط من توقف القلب مع الإنعاش القلبي الرئوي المستمر1. الأسباب الأكثر شيوعا ل CS هي MI الحاد (AMI) التي تمثل 81٪ من الحالات في تحليل تم الإبلاغ عنه مؤخرا2 ، وفشل القلب الحاد المعوض (ADHF). يتميز CS تقليديا بالاحتقان وضعف التشوه ، والذي يتجلى في ضغوط التعبئة المرتفعة (ضغط إسفين الشعيرات الدموية الرئوية [PCWP] ، والضغط البطيني الأيسر النهائي الانبساطي [LVEDP] ، والضغط الوريدي المركزي [CVP] ، والضغط الانبساطي البطيني الأيمن [RVEDP]) ، وانخفاض الناتج القلبي (CO) ، ومؤشر القلب (CI) ، وإخراج الطاقة القلبية (CPO) ، وعطل الجهاز النهائي3 . في الماضي ، كانت العلاجات الوحيدة المتاحة ل AMI المعقدة بسبب CS هي إعادة الأوعية الدموية المبكرة والإدارة الطبية مع inotropes و / أو vasopressors4. وفي الآونة الأخيرة، ومع ظهور أجهزة دعم الدورة الدموية الميكانيكية والاعتراف بأن تصاعد أجهزة ضغط الأوعية يرتبط بزيادة معدل الوفيات، حدث تحول نموذجي في علاج كل من AMI و ADHF CS5،6 ذات الصلة.
في العصر الحالي من أجهزة المساعدة البطينية عن طريق الجلد (pVAD) ، هناك عدد من منصات /تكوينات أجهزة MCS المتاحة ، والتي توفر دعما أحادي البطين أو ثنائي البطين والدورة البطينية مع وبدون القدرة على الأوكسجين7. وعلى الرغم من الزيادات المطردة في استخدام ال PVADs لعلاج كل من AMI و ADHF CS، ظلت معدلات الوفيات دون تغيير إلى حد كبير5. مع ظهور أدلة على الفوائد السريرية المحتملة لتفريغ البطين الأيسر (LV) في AMI8 والاستخدام المبكر ل MCS في AMI CS9 ، يستمر استخدام MCS في الزيادة.
يتجاوز جهاز MCS Atrial to Femoral Arter Bypass (LAFAB) الأيسر الأذين عن طريق تصريف الدم من الأذين الأيسر (LA) وإعادته إلى الدورة الدموية الشريانية الجهازية عبر الشريان الفخذي (الشكل 1). وهو مدعوم بمضخة طرد مركزي خارجية توفر تدفق 2.5-5.0 لتر في الدقيقة (L/m) (مضخة الجيل الجديد ، المعينة باسم LifeSPARC ، قادرة على تدفق يصل إلى 8 لتر / متر) اعتمادا على حجم القنية. بمجرد استخراج الدم من لوس انجليس عن طريق القنية الوريدية عبر الصفاز ، فإنه يمر عبر مضخة الطرد المركزي الخارجية التي تعيد تدوير الدم مرة أخرى إلى جسم المريض عن طريق القنية الشريانية الموضوعة في الشريان الفخذي.
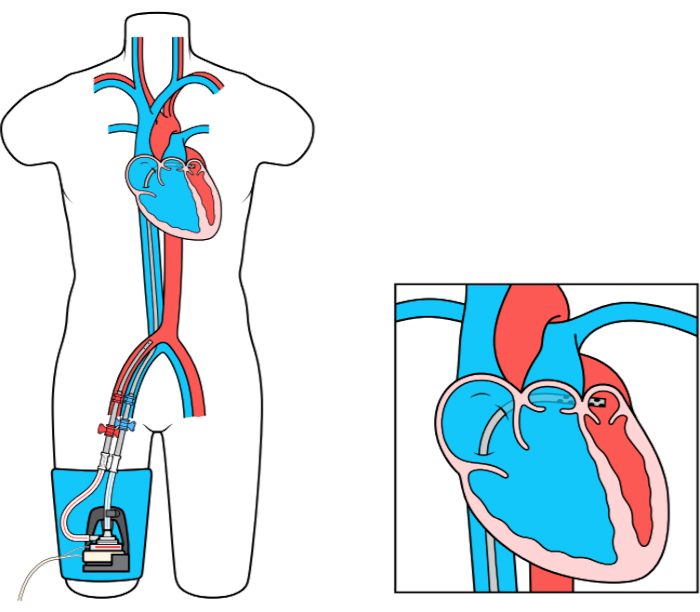
الشكل 1: إعداد LAFAB. صورة مجاملة من TandemLife ، وهي شركة تابعة مملوكة بالكامل لشركة LivaNova US Inc. يرجى النقر هنا لعرض نسخة أكبر من هذا الرقم.
