कार्डियोजेनिक शॉक (सीएस) सहवर्ती हाइपोटेंशन के साथ या बिना ऊतक हाइपोपरफ्यूजन की एक स्थिति है, जिसमें हृदय शरीर की मांगों को पूरा करने के लिए पर्याप्त रक्त और ऑक्सीजन देने में असमर्थ होता है, जिसके परिणामस्वरूप अंग विफलता होती है। इसे सोसाइटी ऑफ कार्डियोवैस्कुलर एंजियोग्राफी एंड इंटरवेंशन्स (एससीएआई) द्वारा ए से ई तक चरणों में वर्गीकृत किया गया है: चरण ए – सीएस के लिए जोखिम वाले रोगी; चरण बी – हाइपोपरफ्यूजन के बिना हाइपोटेंशन या टैचीकार्डिया के साथ सीएस के शुरुआती चरण में रोगियों; चरण सी – ठंडे और गीले फेनोटाइप के साथ क्लासिक सीएस को परफ्यूजन बनाए रखने के लिए इनोट्रोप्स / वैसोप्रेसर्स या यांत्रिक समर्थन की आवश्यकता होती है; चरण डी – वर्तमान चिकित्सा या यांत्रिक समर्थन पर बिगड़ना अधिक उन्नत उपकरणों के लिए वृद्धि की आवश्यकता होती है; और चरण ई – परिसंचरण पतन और दुर्दम्य अतालता के साथ रोगियों को शामिल किया गया है जो सक्रिय रूप से चल रहे कार्डियोपल्मोनरी पुनर्जीवन 1 के साथ कार्डियक गिरफ्तारी का अनुभव कर रहे हैं। सीएस के सबसे आम कारण तीव्र एमआई (एएमआई) हैं जो हाल ही में रिपोर्ट किए गए विश्लेषण 2 में 81% मामलों का प्रतिनिधित्व करते हैं, और तीव्र विघटित दिल की विफलता (एडीएचएफ)। सीएस शास्त्रीय रूप से भीड़ और बिगड़ा हुआ परफ्यूजन की विशेषता है, जो ऊंचा भरने के दबाव (फुफ्फुसीय केशिका कील दबाव [PCWP], बाएं वेंट्रिकुलर एंड-डायस्टोलिक दबाव [एलवीईडीपी], केंद्रीय शिरापरक दबाव [सीवीपी], और दाएं वेंट्रिकुलर एंड-डायस्टोलिक दबाव [आरवीईडीपी]), कार्डियक आउटपुट (सीओ), कार्डियक इंडेक्स (सीआई), कार्डियक पावर आउटपुट (सीपीओ), और अंत-अंग खराबी 3 द्वारा प्रकट होता है। . अतीत में, सीएस द्वारा जटिल एएमआई के लिए एकमात्र उपलब्ध उपचार शुरुआती पुनर्संवहनीकरण और इनोट्रोप्स और / या वैसोप्रेसर्स 4 के साथ चिकित्सा प्रबंधन थे। हाल ही में, यांत्रिक परिसंचरण समर्थन (एमसीएस) उपकरणों के आगमन और मान्यता के साथ कि वैसोप्रेसर्स की वृद्धि बढ़ी हुई मृत्यु दर से जुड़ी हुई है, एएमआई और एडीएचएफ से संबंधित सीएस 5, 6 दोनों के उपचार में एक प्रतिमान बदलाव हुआ है।
Percutaneous वेंट्रिकुलर सहायता उपकरणों (pVAD) के वर्तमान युग में, कई MCS डिवाइस प्लेटफ़ॉर्म / कॉन्फ़िगरेशन उपलब्ध हैं, जो univentricular या biventricular circulatory और वेंट्रिकुलर समर्थन प्रदान करते हैं और ऑक्सीजनेशन क्षमता के बिना। एएमआई और एडीएचएफ सीएस दोनों के इलाज के लिए पीवीएडी के उपयोग में लगातार वृद्धि के बावजूद, मृत्यु दर काफी हद तक अपरिवर्तित रही है5। एएमआई 8 में बाएं वेंट्रिकल (एलवी) के शुरुआती अनलोडिंग और एएमआई सीएस 9 में एमसीएस के शुरुआती उपयोग के लिए संभावित नैदानिक लाभों के लिए उभरते सबूतों के साथ, एमसीएस का उपयोग बढ़ रहा है।
बाएं अलिंद से फेमोरल आर्टरी बाईपास (एलएएफएबी) एमसीएस डिवाइस बाएं आलिंद (एलए) से रक्त निकालकर एलवी को बाईपास करता है और इसे ऊरु धमनी (चित्रा 1) के माध्यम से प्रणालीगत धमनी परिसंचरण में वापस कर देता है। यह एक बाहरी केन्द्रापसारक पंप द्वारा समर्थित है जो 2.5-5.0 लीटर प्रति मिनट (एल / एम) प्रवाह (नई पीढ़ी के पंप, जिसे लाइफस्पार्क के रूप में नामित किया गया है, जो 8 एल / एम प्रवाह तक सक्षम है) प्रदान करता है, जो कैनुला के आकार पर निर्भर करता है। एक बार जब रक्त ट्रांससेप्टल शिरापरक कैनुला के माध्यम से एलए से निकाला जाता है, तो यह बाहरी केन्द्रापसारक पंप से गुजरता है जो ऊरु धमनी में रखी धमनी प्रवेशनी के माध्यम से रोगी के शरीर में रक्त को वापस कर देता है।
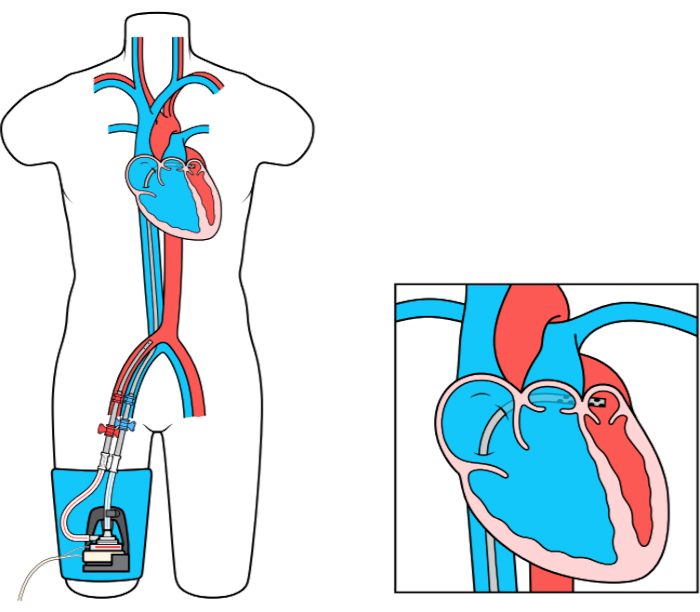
चित्रा 1: LAFAB सेटअप. TandemLife की छवि सौजन्य, LivaNova US Inc की एक पूर्ण स्वामित्व वाली सहायक कंपनी कृपया इस आंकड़े का एक बड़ा संस्करण देखने के लिए यहां क्लिक करें।
