Decellularization
DAPI staining shows the absence of DNA, and no DNA values higher than 50 ng were detected in any of the tracheae any by electrophoresis, with all fragments being smaller than 200 bp20.
Microbial culture
Two of the eight pieces subjected to 0.5 kGy showed color change in less than 1 week. None of the pieces irradiated at 1 kGy and 2 kGy showed any color change (Figure 1).
Histological analysis
No changes to the collagen or elastic fiber distribution pattern were detected in any of the specimens analyzed (Figure 2).
Determining the radiation dose
Given the results described above, which showed that irradiation at 0.5 kGy did not ensure sterilization of the specimen, whereas doses of 1 kGy and 2 kGy did, we established the minimum possible irradiation dose to achieve sterilization of the tissue as 1 kGy. Therefore, we tested the biomechanical impact of this dose on the tracheas2,17,23.
Biomechanical study
Axial tensile tests
The data obtained in the tensile test on irradiated tracheas are shown in Table 1. Figure 3 shows the corresponding stress-strain curves and breaking points.
Thus, subjecting tracheal pieces to gamma irradiation for sterilization purposes, despite slightly increasing the detected values, does not cause significant effects on the axial biomechanical characteristics of the organs. Hence, both the σmax that the tracheas can tolerate (0.05 MPa; CI [-0.046, 0.144] MPa), as well as εmax (0.096 CI [-0.096, 0.281]), (0.022 MPa; CI [-0.23, 0.274] MPa), and W / Vol (from 0.044 mJ / mm3; CI [-0.018, 0.106] mJ/mm3), are very slightly increased in this sample, but are not in any case applicable to the population estimate.
Radial compression tests
The compression tests performed on both the native tracheas (controls) and on the decellularized, cryopreserved, and irradiated tracheas are shown in Table 2. The corresponding graphs can be seen in Figure 4.
Gamma irradiation causes only a minimal but significant decrease in radial biomechanical characteristics in the variable force per unit of length, which varies by -0.017 N/mm; CI [-0.042, -0.004] N/mm, while the minimal variations detected in W/Vol (0.044 mJ/mm3; CI [-0.018, 0.106] mJ/mm3), R (-0.018 MPa · mm; CI [-0.145, 0.083] MPa · mm), and W/S (-0.081 mJ/mm2; CI [-0.95, 0.74] mJ/mm2), are in no case applicable to the population estimate (Figure 5).
Implant
Macroscopic examination
None of the animals showed inflammatory or infectious symptoms during the postoperative period; their diet was reinstated as planned and antibiotics and analgesics were suspended on day five. Upon euthanasia, integration of the trachea and the flap was observed macroscopically, with no visible signs of inflammation.
Histological examination
The histological examination showed the flap forming highly organized connective tissue – closely linked to the tracheal rings, showing continuity between them and the tissue – in the form of the perichondrium of the native trachea. The cartilage was intact and showed no signs of necrosis. In addition, the presence of macrophages and some isolated giant cells forming sheets were observed. Other than the scarce presence of eosinophils, usual postsurgical mild acute inflammatory cellularity was observed (Figure 6). Incipient neovascularization was also observed around the trachea.
Biomechanical evaluation
After being implanted in the lagomorph, the characteristics of the trachea remained unchanged, except for the force per unit length, which recovered the characteristics of the native trachea only 2 weeks after the transplant (0.006 N/mm, CI [-0.026, 0.04] N/mm) (Figure 7).
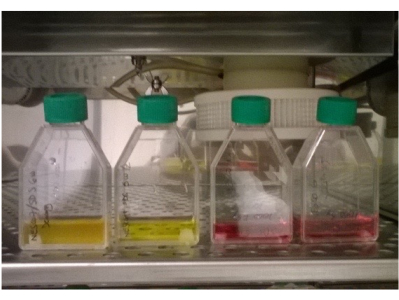
Figure 1: Irradiated tracheas in DMEM without antibiotics or antifungals. The color of the two specimens on the left (0.5 kGy) has changed, indicating a change in pH, and is an indirect sign of bacterial growth. There is also increased turbidity in the first specimen on the left. The two specimens on the right (1 kGy) show no color change. Please click here to view a larger version of this figure.
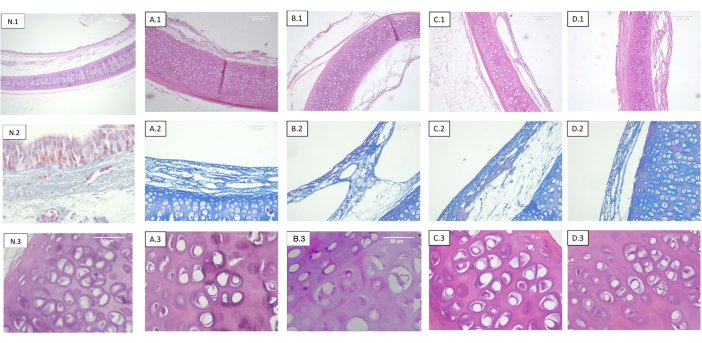
Figure 2: Tracheas decellularized and irradiated at different doses. Each row corresponds to a different staining and each column to different sterilization dosage. 1) Hematoxylin-eosin. Panoramic view of the cartilage, mucosa, submucosa, and serosa. 2) Masson's trichrome stain. Tracheal submucosa. 3) Hematoxylin-eosin. Detailed view of the tracheal cartilage. (A) Non-irradiated tracheas (control). (B) Tracheas irradiated at 0.5 kGy. (C) Tracheas irradiated at 1 kGy. (D) Tracheas irradiated at 2 kGy. The absence of objective histological changes with respect to the radiation dose is observed. Abbreviation: N = native trachea. Please click here to view a larger version of this figure.
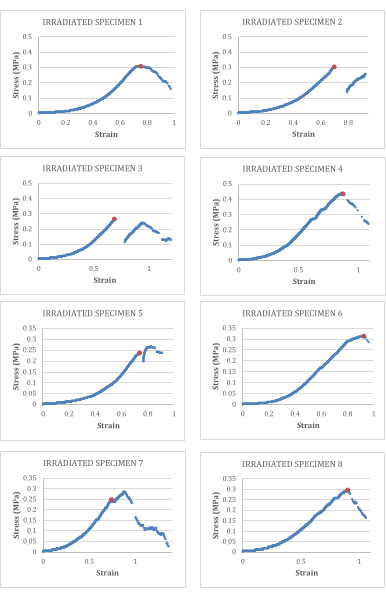
Figure 3: Stress-strain curves for decellularized and irradiated tracheas. The breaking point is marked in orange. Please click here to view a larger version of this figure.
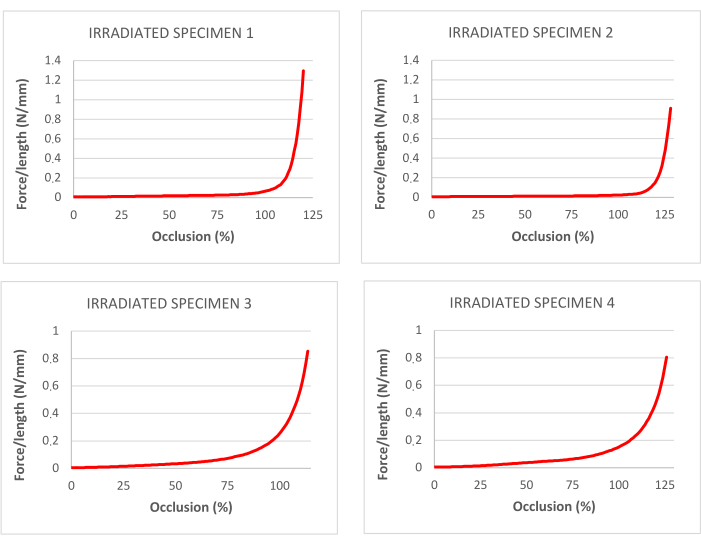
Figure 4: curves for percentage of occlusion corresponding to traction tests in decellularized and irradiated tracheas. Please click here to view a larger version of this figure.
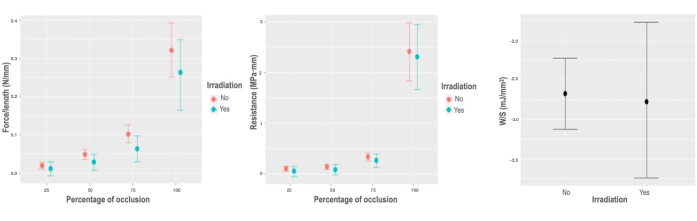
Figure 5: Biomechanical response to irradiation. (A) Graph of marginal effects on the variable force per unit of length, according to the percentage of occlusion of the irradiation interaction. (B) Graph of marginal effects on the variable force per unit of length, according to the percentage of occlusion of the irradiation interaction. (C) Partial dependence plot of the stored energy per unit area model for the irradiation variable. Please click here to view a larger version of this figure.
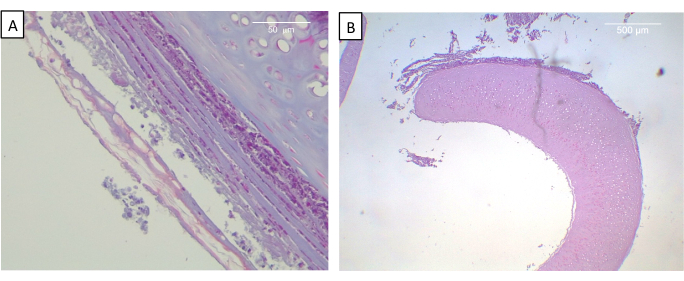
Figure 6: View of implanted trachea at 2 weeks. (A) Masson's trichrome staining. Neoformed connective tissue of the tracheal outer surface organized in concentric layers of fibers and cells is observed. (B) Hematoxylin-eosin. Panoramic view of perfectly preserved cartilage. Please click here to view a larger version of this figure.
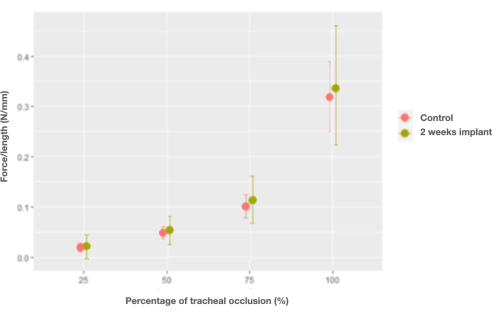
Figure 7: Graph of the marginal effects of the interaction between force per unit length and percentage of occlusion and control (native) tracheas versus trachea implants at 2 weeks. Please click here to view a larger version of this figure.
Table 1: Tensile tests on irradiated tracheas. Controls are native rabbit tracheas. Please click here to download this Table.
Table 2: Compression tests on irradiated, decellularized tracheas. Controls are native rabbit tracheas. Please click here to download this Table.
