General conditions
The mean operative time for the SG procedure was 49.3 ± 1.5 min. We removed 62.8 ± 5.0 mg of stomach, which represents about 80% percent of the stomach. No mice died during the surgery or during the following seven days. One mouse (7.1%) died on the 11th postoperative day because of a gastric obstruction caused by a bezoar.
The mean operative time for the RYGB procedure was 89.1 ± 2.8 min. The mortality rate was significantly higher after RYGB (sham: 25% versus RYGB: 66.6%; p = 0.038). The main causes of postoperative deaths were anastomotic leaks (n = 8), anastomotic stenosis (n = 5), anesthesia complications (n = 4), and postoperative bleeding (n = 2). We also observed two long-term deaths due to gastrointestinal anastomosis stenosis with chronic obstruction and malnutrition. As shown in Figure 3, we noticed a progressive improvement of the post-operative survival rate throughout the protocol, indicating that intensive surgical training is required to master the RYGB surgical technique.
Body weight, food intake, and glucose homeostasis
The mice had similar body weights before surgery. SG demonstrated significant weight loss 14 days after surgery compared to sham control mice (sham: -6.6% versus SG: -16.0%; p <0.01; Figure 4A). RYGB was associated with significant weight loss from postoperative days 14 (sham: -7.9% on day 14 post-surgery and -5.1% on day 28 post-surgery versus RYGB: -22.9% on day 14 post-surgery and -25.5% on day 28 post-surgery; Figure 4B). The daily food intake was reduced by 35% during the 14-day period following the SG (Figure 4C). In contrast, we did not observe such an anorexigenic effect between the sham and RYGB mice (Figure 4D). We also reported an improvement of glucose tolerance following SG and RYGB surgeries (Figure 4E, 4F).
Beneficial effect of iron supplementation on RYGB-induced anemia
We did not observe a significant decrease of hemoglobinemia 14 days after SG surgery (data not shown). In contrast, severe anemia was measured in RYGB-operated mice, but it did benefit from specific iron supplementation (Figure 5A). Daily iron supplementation was indeed crucial and prevented significant anemia 28 days after RYGB surgery (Figure 5B).
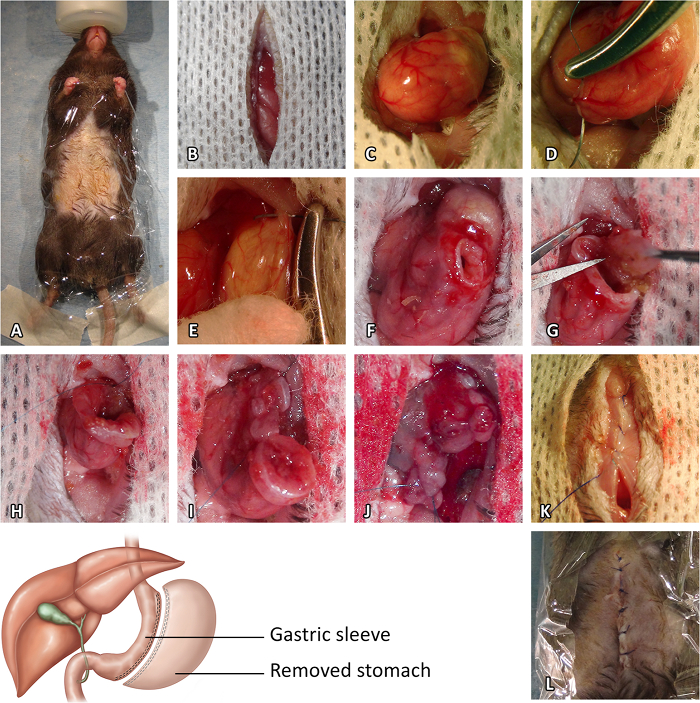
Figure 1: Sleeve Gastrectomy Procedure. (A) Preoperative preparation. (B) Median laparotomy. (C) Stomach exposure. (D) Pylorus vessel suture. (E) Esophagus vessel suture. (F) Initial gastrotomy. (G) Resection of the cardiac region of the stomach. (H) Closure of the stomach opening from the gastroesophageal junction to the end of the incision. (I) Resection of the pyloric region of the stomach. (J) Closure of the opening of the pyloric region. (K) Closure of the muscle layer of the abdominal wall. (L) Closure of the skin. Please click here to view a larger version of this figure.
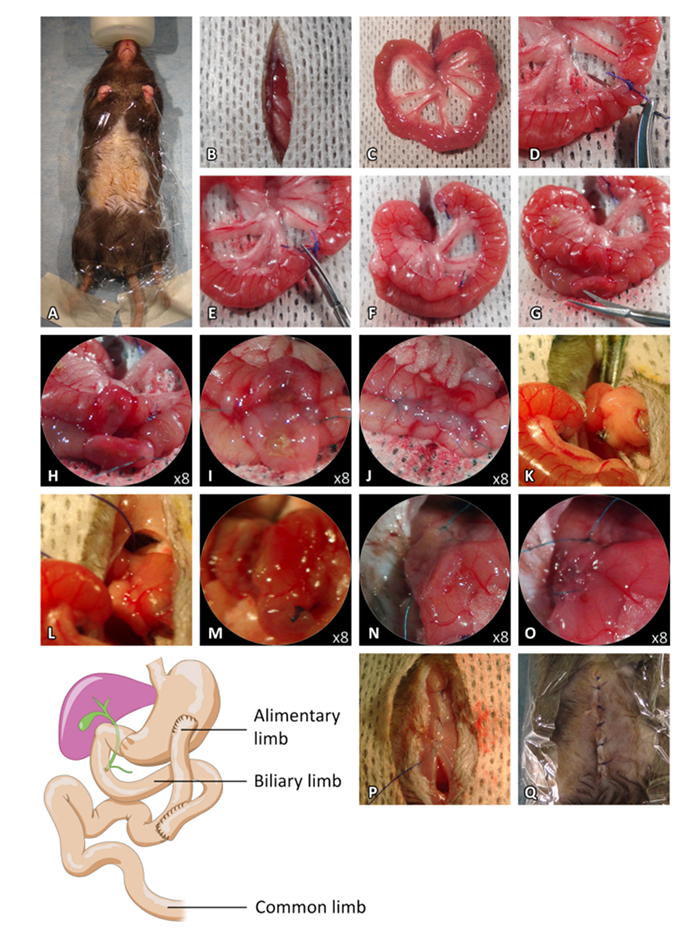
Figure 2: Roux-en-Y bypass Procedure. (A) Preoperative preparation. (B) Median laparotomy. (C) Externalization of the small intestine. (D) Biliopancreatic and alimentary limbs ligatures. (E) Small intestine section between the ligature. (F) Intestinal limb positioning for the jejuno-jejunostomy. (G–H) Antimesenteric incisions of the proximal limb and the intestine loop. (I) Dorsal side-to-side anastomosis. (J) Ventral side-to-side anastomosis. (K–L) Pylorus ligature. (M) Incision of the ventral side of the stomach. (N) Incision of the distal limb and dorsal side-to-side anastomosis. (O) Ventral side-to-side anastomosis. (P) Closure of the muscle layer of the abdominal wall. (Q) Closure of the skin. Please click here to view a larger version of this figure.
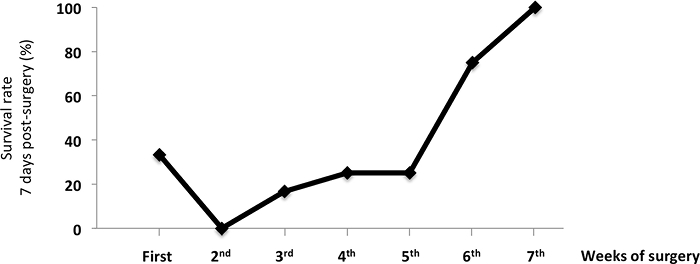
Figure 3: Survival Rate of Mice 7 Days after the RYGB Surgery. The data show the benefit of surgical training on the survival rate of RYGB-operated mice. The values are shown as the mean value ± SEM. Please click here to view a larger version of this figure.
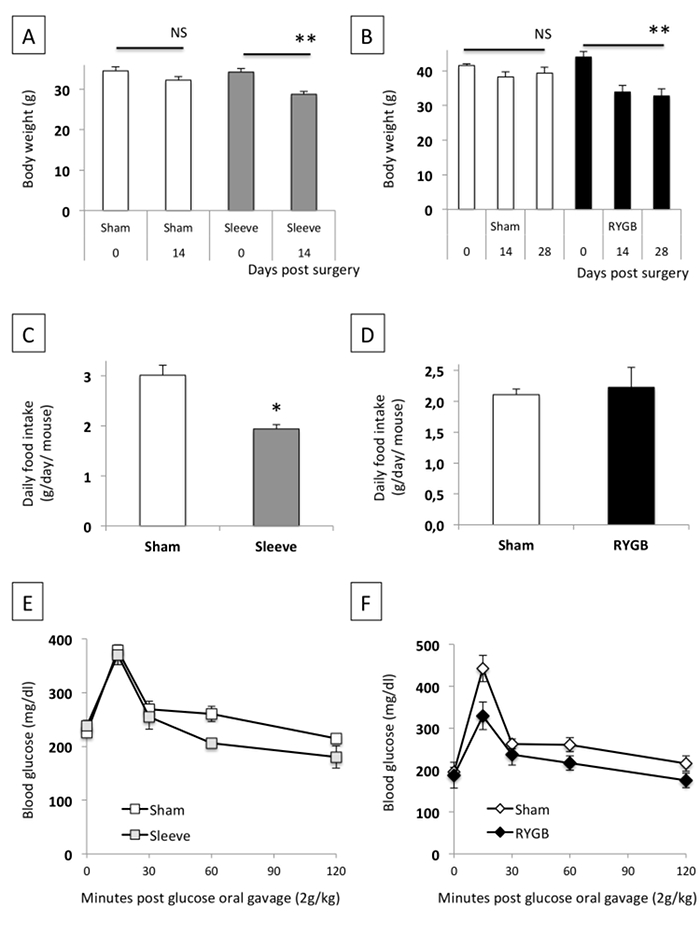
Figure 4: Effect of SG (A, C, D) and RYGB (B, D, F) on Bodyweight, Daily Food Intake, and Glucose Tolerance. The data are shown as the mean value ± SEM. NS: not significant; * P <0.05; ** P <0.01 (Mann-Whitney test, ANOVA test). Please click here to view a larger version of this figure.
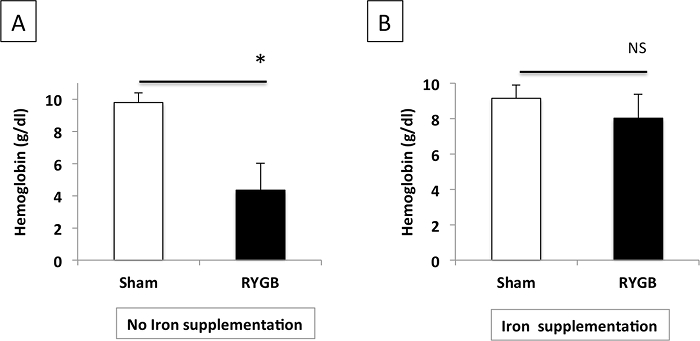
Figure 5: Plasma Hemoglobin Levels after RYGB in Mice Without (A) or With (B) Iron Supplementation. The data are shown as the mean value ± SEM. NS: not significant; * P <0.05 (Mann-Whitney test). Please click here to view a larger version of this figure.
