To confirm the robustness of adapting this infection model to 96-well plate format, we here examined the drug susceptibility of Mtb derived from our 96-well adapted infection model to rifampicin (RIF) and moxifloxacin (MOXI) according to the template given in Figure 1A. We demonstrate that the generation of Mtb/macrophage aggregate structures key to this assay can be reliably produced in a 96-well plate format (Figure 2), thereby enabling throughput compatibility (Figure 1B). Macrophage passaged Mtb produced in this manner can be directly used for drug efficacy testing using the well characterized resazurin microtiter assay (Figure 3).
As the resazurin assay relies on the oxidative species produced by metabolically active Mtb to convert the blue resazurin to the fluorescent pink resorufin, the change in color and fluorescence can be used to as a surrogate marker to determine the amount of bacterial growth. In Figure 3A, we show that there is enough sensitivity within the resazurin assay to reliably detect viable Mtb bacteria capable of replicating in the absence of drugs after only 3 days of incubation. While visual confirmation of endpoint color change is only an approximate evaluation of growth, we can accurately quantify this by kinetically measuring the conversion of resazurin to its fluorescent metabolite resorufin using a plate reader (Figure 3B). Using these data, normalizing to the positive growth control (absence of drugs) allows for the computation of susceptibility killing curves to visualize drug efficacy against macrophage-passaged Mtb (Figure 4).
Here, the representative results in Figures 3 and 4 show that the minimal inhibitory concentration (MIC), defined as the lowest concentration of the antibiotic at which 90% growth inhibition is observed, is greater than 2 µg/mL for both rifampicin and moxifloxacin against Mtb derived from our infection model. This demonstrates that our infection model predicts efficacy of anti-Mtb drugs that are more in line with MIC values determined against intracellular Mtb8, and thus reflects the diffusion barrier properties that are neglected in most Mtb drug susceptibility assays using broth grown bacterial cells.
Importantly, the data obtained using the described assay in 96-well format showed highly comparable results to those we had previously determined for rifampicin and moxifloxacin against macrophage-passaged Mtb16.
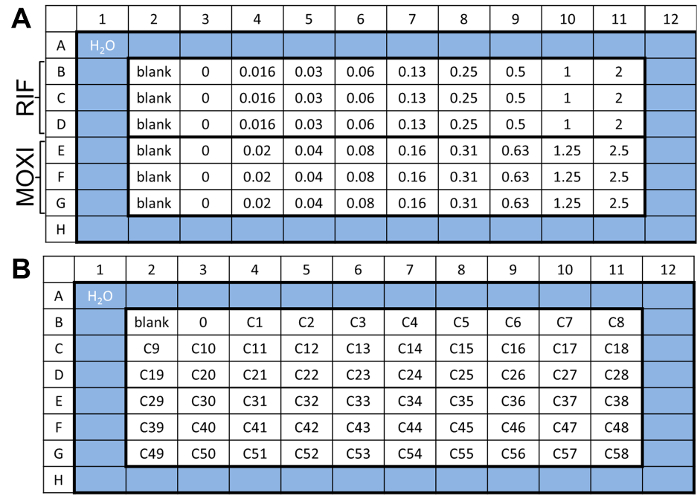
Figure 1: Drug plate layout. (A) Example template of the drug challenge plate used in step 4. This allows for the parallel testing of two drugs in triplicate wells at 8 defined concentrations. As a representative experiment, we used rifampicin (RIF) and moxifloxacin (MOXI) starting at 2 µM and 2.5 µM, respectively. (B) An alternative template for throughput screening is also provided to show the possibility of testing of 58 compounds at a single concentration. Please click here to view a larger version of this figure.
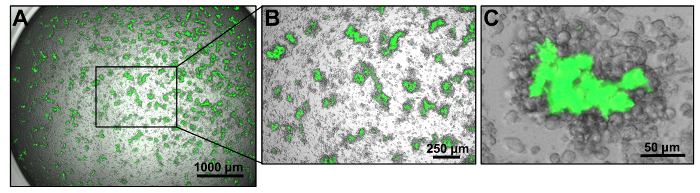
Figure 2: Generation of Mtb/macrophage aggregate structures in 96-well plate format. (A) Representative bright field and GFP merged images of Mtb-macrophage aggregates on Day 9 post infection. Images were captured with a 4X objective using an automated cell imaging program that documents the entire well by stitching a montage of 3 by 3 individually captured images. (B) An individual non-stitched image from the visual field shown in (A). (C) A representative merged bright field and GFP image of an Mtb/macrophage aggregate structure captured with a 10X objective. Please click here to view a larger version of this figure.
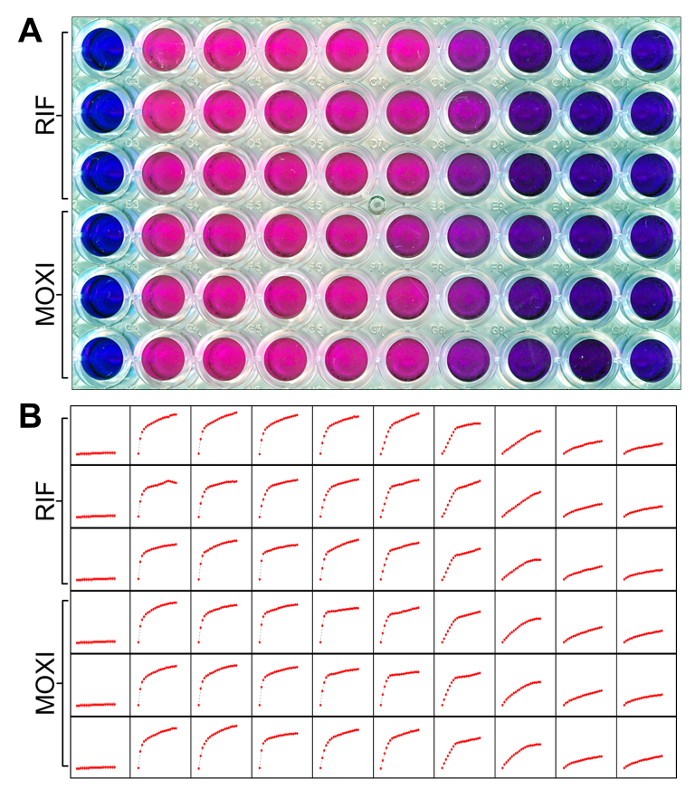
Figure 3: Using the resazurin microtiter assay to measure Mtb viability. (A) The presence of viable Mtb cells can be simply determined by the conversion of the blue resazurin dye to its pink, reduced form. Representative results are shown here using rifampicin (RIF) and moxifloxacin (MOXI) according to the template in Figure 1A. (B) To quantitatively measure the conversion of resazurin, fluorescence of individual wells (corresponding to Figure 3A) was monitored kinetically for 24 h as described in step 5. Representative mini-graphs show relative fluorescence units (y-axis) versus time (x-axis). Please click here to view a larger version of this figure.
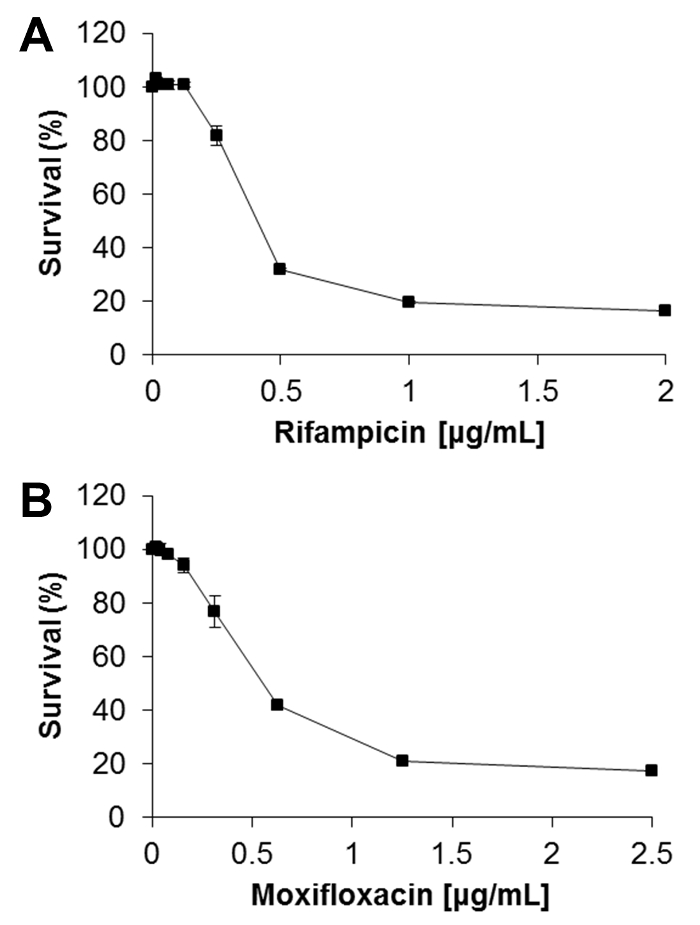
Figure 4: Determining drug susceptibility killing curves from REMA data. Relative fluorescence units at the time of maximal resazurin signal in (A) rifampicin and (B) moxifloxacin treated wells (from Figure 3B) were normalized to the no drug control (maximal Mtb growth) as 100% survival. Background control (Blank) signals were subtracted from every sample well. The percent survival was plotted for each individual concentration of drug treatment to generate a killing curve. Data in this figure represent the means ± S.D. of three independent experiments. Please click here to view a larger version of this figure.
