Cancer and biomarker research relies on a supply of quality human tissue samples, and limited supply has hindered research1,2. Many dermatologic studies are limited by the inadequate supply, variable quality, and costs associated with the use of human tissue. The cost of establishing a large, dedicated biobank has been estimated to be approximately two million dollars3, and these costs place the use of human tissue out of the reach of many researchers. Furthermore, the process of generating and storing research samples poses the risk of affecting clinical operations and delaying patient care if not carefully executed. A cost-effective, clinic-based biorepository has been established that focuses on skin cancer samples following recommended best practices and sample validation4,5,6.
This protocol has been developed in a dermatology clinic that performs a large volume of Mohs micrographic surgeries to remove squamous cell carcinoma (SCC), basal cell carcinoma (BCC), and melanoma skin cancers. Volunteer donors can be recruited from this patient population. It is important to establish the biorepository at the site of collection to rapidly capture tissue and blood from consented patients without delaying treatment. Gathering samples from the same clinic minimizes variations in collection techniques and minimizes variations in the quality of samples, which can be problematic for downstream applications7,8.
The goal of the Mohs micrographic surgery technique is to ensure that all cancer tissue is removed while preserving as much healthy tissue as possible. The procedure involves the progressive removal of thin layers of tumor tissue. Each successive layer is histologically examined (after cryosectioning the tumor tissue and performing H&E staining) by a dermatologist to determine if all cancer tissue has been removed. The excision and examination of subsequent layers of tissues is executed while the patient remains in the office. This technique is considered the best treatment option for SCC9. At this point, the wound is closed and, to improve healing and cosmetic appearance, adjacent normal tissue (ANT) is frequently excised. Thus, this surgical procedure to remove a tumor is ideally suited for collecting histologically characterized tissue for future studies.
The procurement procedure for obtaining tumor tissue, adjacent normal tissue, saliva, and blood samples has been designed to have minimal impact on normal staff duties (Figure 1). Medical assistants perform the blood draws while preparing the patient for the procedure. After completion of the Mohs procedure, the Mohs histotechnologist prepares additional histological slides of the specimen and transfers the tissue to the biorepository. Costs associated with establishing the biorepository include the purchase of cryopreservation freezers, the creation of modest clinical laboratory space, and the development of an inventory tracking program.
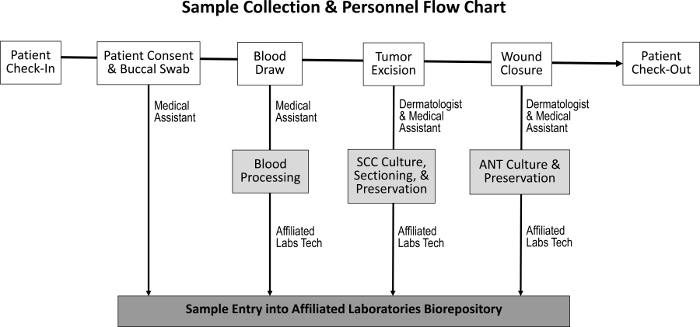
Figure 1: Sequence of sample collection and responsible staff. Upon patient check-in and the attainment of patient consent, the medical assistant collects a buccal swab and performs a blood draw. The dermatologist and medical assistant then excise the tumor and close the wound, during which time SCC and ANT specimens are collected, respectively. A dedicated laboratory technician processes the blood and sections the SCC and ANT specimens for tissue culture, preservation, and entry into the biorepository. Please click here to view a larger version of this figure.
The diversity of samples collected enables a variety of experimental approaches (Figure 2). Samples collected from the patient are buccal swabs (saliva can also be collected if needed), whole blood, and excised tissue. The buccal swabs and a sample from the whole blood are saved, without processing, for genotyping and tissue matching. Whole blood is separated into white blood cell (WBC) and plasma fractions for future analyses. After Mohs processing, the frozen tumor is placed directly into liquid nitrogen and transferred to a -80 °C freezer. Fresh, viable tumor tissue and ANT samples are cultured using modifications of previous techniques10,11 and then cryopreserved. During collection, the number of each sample type is recorded on a spreadsheet prior to entry into the inventory tracking program to facilitate accurate processing (Table 1).
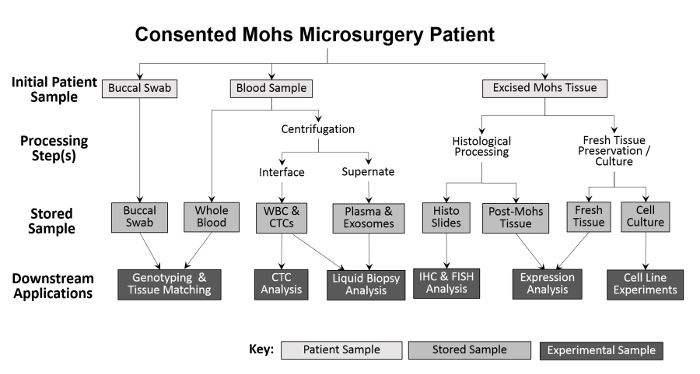
Figure 2: Outline of clinic-based biorepository sample collection and processing. A buccal swab and blood sample are collected from the patient and stored for downstream genotyping and tissue matching. Whole blood is further processed for white blood cell (WBC) isolation and CTC analysis, as well as for plasma collection and liquid biopsy analysis. Tissue excised during the Mohs procedure is histologically processed for diagnostic purposes, after which the histologic slides can be used experimentally for further immunohistochemical analyses. Provided that the excised tissue sample is large enough, a portion of fresh tissue is removed and sectioned for protein and RNA isolation, and for the establishment of cultured cell lines. Please click here to view a larger version of this figure.
| Collection Date: | |||||
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | |
| Initials and Birth Date | |||||
| Eye Color | |||||
| Sample Type | |||||
| Sample Location | |||||
| Saliva | |||||
| Whole Blood | |||||
| Plasma | |||||
| Tumor Viable | |||||
| Tissue Normal Viable | |||||
| Tumor Mohs Liquid Nitrogen | |||||
| Tissue Normal Liquid Nitrogen | |||||
| Slides |
Table 1: Checklist to record sample collections. Data tracked and recorded with each sample collected include patient initials, birth date, and eye color (for skin typing), as well as the location of specimen removal. The number of saliva samples, blood collection volumes, and the number of viable and preserved tissue specimens collected are also recorded as references for allocations to later uses. Please click here to download this file.
To validate sample collection procedures, each sample type has been tested in downstream applications. Using modifications of previous techniques12, tumor and ANT have been successfully used in protein and RNA isolation and can potentially be used for DNA isolation. Viable explants established from the tissue sections have been evaluated by microscopy, while stored histological slides have been used for immunohistochemistry and immunofluorescence.
By following the protocol described here, it is possible to extend this model to other dermatology clinics, other tumor types (such as melanoma), and other surgical specialties and practices to provide human tissue samples for multifaceted research into human cancers. Slight modifications of this protocol are likely to be necessary for other practices but, in principle, this protocol is applicable to any surgical practice that routinely discards patient samples gathered in the course of patient treatment.
Tumor and ANT have been used successfully in protein isolation and tested by Western blotting. As shown in Figure 3, cutaneous squamous cell carcinoma markers (Muc114, FHL-115, and p4016,17) can be detected in patient samples collected and stored in our clinic-based biorepository.
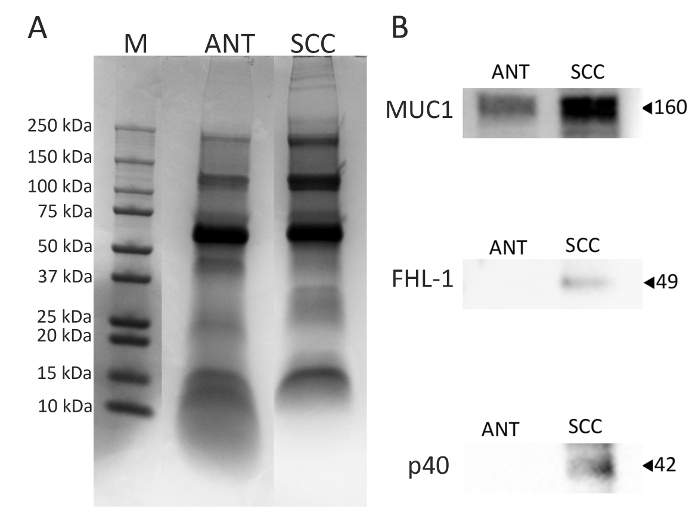
Figure 3: Analysis of proteins extracted from ANT and SCC. Total protein was isolated from ANT and SCC samples, and the expression of known markers for SCC were examined by Western blot. Representative Western blots of mucin 1 (MUC1), Factor H Like-1 (FHL-1), and p40 (panel B) are shown. Please click here to view a larger version of this figure.
RNA isolated using the above techniques has been tested by gel electrophoresis, qPCR, and RNA integrity analysis. Figure 4 shows two patient samples from which high-quality, intact RNA was isolated. The RNA is suitable for all downstream applications.
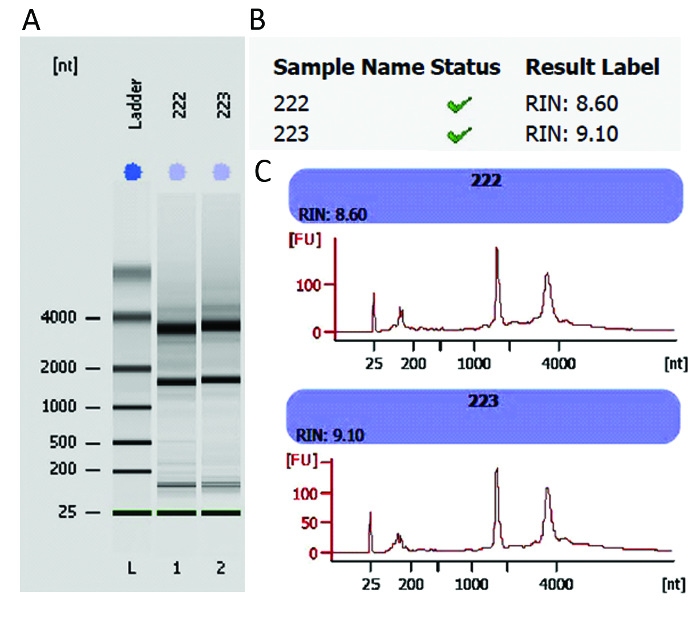
Figure 4: RNA integrity analysis using bioanalysis. Assessment of RNA size and integrity by gel electrophoresis (panel A). An RNA integrity number (RIN) was generated for each sample based on the electrophoretic trace of the RNA sample, including the ratio of ribosomal RNA and the presence or absence of degradation products (panel B). An RIN of "10" represents a perfect RNA sample, without any degradation products, whereas "1" marks a completely degraded sample. Densitometry profiles of the bands are plotted as fluorescence units (FU) versus nucleotides (nt) (panel C) for representative RNA samples from SCC and ANT patient tissue. Please click here to view a larger version of this figure.
Viable explants established from the tissue sections have been evaluated by microscopy (Figure 5A). These explant cultures, generated from tumor and ANT samples, are mixed keratinocyte and fibroblast cultures. These cultures may be subcultured or used for future cell line development. Stored histological slides have been used for immunohistochemistry and immunofluorescence. Shown in Figure 5B, an SCC sample shows positive staining for an epithelial-to-mesenchymal transition marker in SCC18.
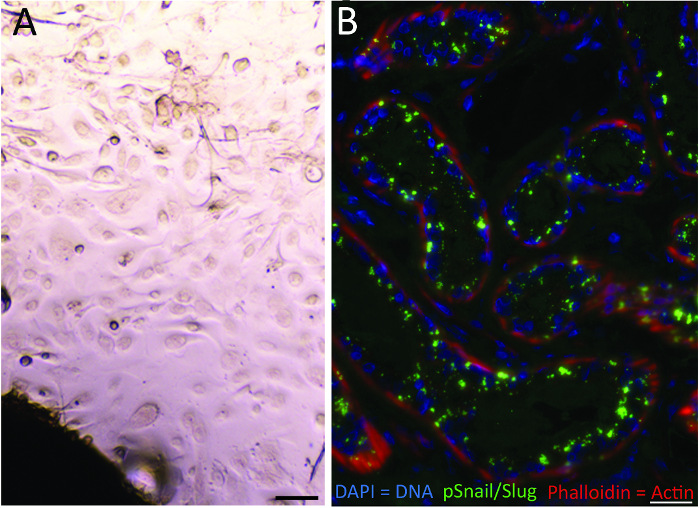
Figure 5: Explant culture and IF staining of SCC sections. Phase contrast image of a squamous cell carcinoma tissue explant (panel A, Scale bar = 50 µm) and tissue sections gathered as part of Mohs micrographic surgery, stained with an anti-pSnail/Slug primary antibody (panel B, Scale bar = 25 µm). Please click here to view a larger version of this figure.
We have experimentally determined that tissue can be stored at 4 °C for 24-48 h prior to RNA isolation (step 5) or explant culture (step 6) without affecting results. RNA yield or integrity, as assessed by gel electrophoresis or bioanalyzer and RIN number, are not compromised. In addition, explant cultures are easily obtained using tissue stored at 4 °C for this length of time. This provides increased flexibility when transferring samples between the clinic and the research lab. As RNA isolation and explant culture are performed in the research lab and not in the clinic, this feature makes the clinic-based biorepository a more robust model than we previously expected.
To the author's knowledge, this protocol is the first of its kind that focuses on the clinical procurement of cutaneous tissue samples in both a cost-effective and fast approach. Patients undergoing Mohs microsurgery are typically scheduled during specific blocks of time, and collection is limited to these periods. Sample collection involves effort from the medical assistant involved in patient care, the Mohs histotechnologist who processes the tumor samples, and a designated laboratory staff member who handles sample entry and blood processing.
With careful coordination between the three members of the collection team (i.e., the medical assistant, Mohs histotechnologist, and laboratory technician), we have found that the existing medical assisting staff can complete the additional tasks associated with the collection of 3-5 tissue samples per day without any apparent delay in clinic operations. Obtaining patient consent and collecting buccal swabs and blood are completed during normal waiting periods involved with the Mohs microsurgery procedure. Other than the decision-making about how a sample is to be processed, the tasks for which the Mohs histotechnologist is responsible are completed at the end of the Mohs processing of patient samples and typically will add approximately 30 min to the daily schedule. Typically, one member of the clinic staff is responsible for labeling and processing the blood samples and for performing any transfer and entry of samples into the database. Depending on the number of samples processed, these duties may require substantial time away from existing duties; thus, sample collection should only be conducted when sufficient laboratory staffing is available. Specifically, if more than 5 samples are collected in a single day, or if several blood samples are collected from patients, several hours of additional effort from the laboratory technician is needed.
On collection days, the medical assistants (MA) obtain consent from the patients for donations of tissue. The MA subsequently obtains a buccal swab (and saliva, if necessary) and collects blood for processing by laboratory personnel. There is no more patient involvement after the collection of these samples, so from the patient's perspective, the remainder of the clinic visit is unchanged (although they are asked to donate blood during any follow-up visit). Currently, we can estimate that 70% of patients consent to donate tissue, with ~30% of those patients also donating blood; 30% decline to participate. Currently, only patients with a biopsy-proven diagnosis of cancer are included in the biorepository. Patients with a known blood-borne communicable disease are excluded.
The laboratory staff member is responsible for coordinating with the other two members of the collection team and records the samples that are collected (Table 1). After an initial sample collection, the completed consent form, blood, and buccal swabs are transferred to the laboratory staff member, and the donor's initials, birthdate, and other pertinent information, such as the sample type, are recorded. This allows for the recording of the numbers and types of samples collected with each patient during the collection procedure. The flow charts summarizing the processing of both SCC tissue (Figure 6) and ANT (Figure 7) are useful tools for the training of new staff in collection procedures.
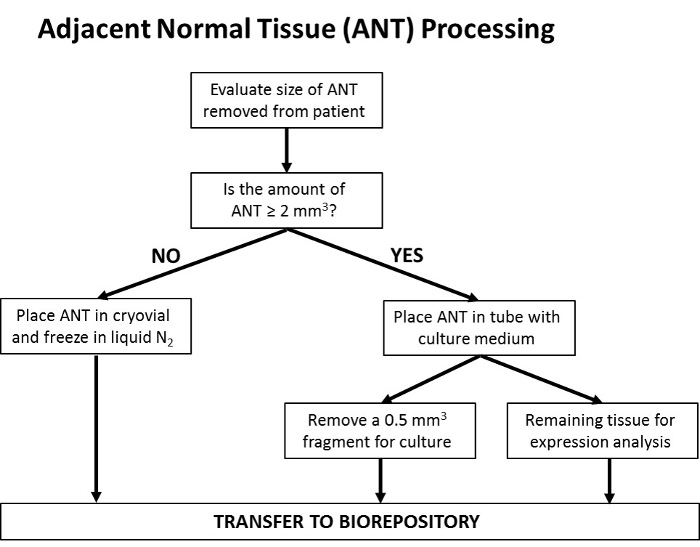
Figure 6: Flowchart delineating the processing of SCC samples. Upon tumor excision, the size of the sample is assessed. If the sample is ≤2 mm3 the entire specimen is utilized for Mohs processing, as the assessment of clean margins (the indication of complete tumor removal) is the top priority. Following Mohs processing, any remaining tissue is frozen in liquid nitrogen and transferred to the biorepository. If the sample is large enough, such that a >2 mm3 portion of the tissue can be removed, this portion is collected and placed in a tube containing cell culture medium, while the remaining portion is utilized for Mohs processing and stored as above. The portion of sample removed to cell culture medium is further segmented, with a ~0.5 mm3 fragment removed and utilized for the establishment of a cell culture line; the remaining tissue fragment is transferred to the biorepository for downstream protein and gene expression analysis. Please click here to view a larger version of this figure.
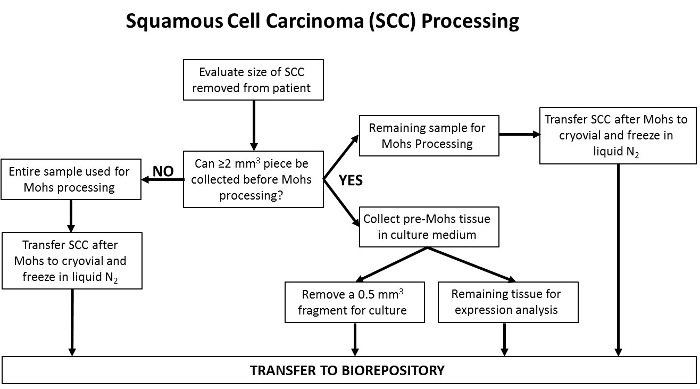
Figure 7: Flowchart delineating the processing of ANT samples. At the time of Mohs closure, a portion of adjacent normal tissue (ANT) is removed and collected by the Mohs surgeon. If the sample size is ≤2 mm3, the entire specimen is placed in a cryogenic tube and frozen in liquid nitrogen before transfer to the biorepository. If the sample is >2 mm3, the entire specimen is first placed into a tube containing cell culture medium. The specimen is then further sectioned into a ~0.5 mm3 fragment, to be used for the establishment of cell culture lines. The remaining tissue section is transferred to the biorepository to be stored for downstream protein and gene expression analysis. Please click here to view a larger version of this figure.
This protocol is designed to minimize variation among samples within the biorepository. Coordination and effective communication among the clinic staff and between the clinic and all laboratory personnel is essential to minimize variability and to maximize the attainment of high-quality DNA, RNA, and protein from the tissues. While the DNA and protein within the tissues are robust, if RNA is desired, it is critical to keep the tissues cold and in the appropriate medium during collection, transport, and processing in order to maintain RNA integrity. Accurate record-keeping is also vital to link the patient samples with their history and diagnosis, as this information is often needed when analyzing results from downstream applications.
With the increasing interest in personalized medicine and biomarker research, a number of biorepositories have recently been established. These are typically associated with hospital-based clinics in large academic centers and have substantial costs involved with setup and operation2,8,19. The development of a clinic-based biorepository for cutaneous cancer samples generated as part of daily practice has several key advantages over other biorepositories. First, with a single collection and sample-processing site, variations in sample handling, which can compromise downstream applications, are minimized. Second, as these donated samples are drawn from a stable patient population, access to de-identified medical records and patient outcome data are unparalleled. These data may be anonymized and transferred from the patient chart to the biorepository database at the time of sample collection or at a follow-up visit. Third, with a loyal patient base, the clinic-based biorepository is able to gather multiple samples from the same patient, a sample set not often obtained in other settings. One of the limitations of this protocol is that it has been optimized for cutaneous samples obtained through Mohs micrographic surgery and may need to be modified for other types of tissues or clinical procedures.
Overall, one of the key goals of the biorepository is to provide a broad spectrum of samples from the same donor to enable researchers to ask a wide range of questions, particularly for the development of liquid biopsies and cancer markers. Specifically, the ability to correlate tumor histology and the expression of biomarkers at the mRNA and protein levels to plasma samples, as well as the ability to reference patient outcome data, creates a uniquely powerful dataset. We hope that the clinic-based biorepository model may be utilized to help alleviate the shortage of patient samples in biomedical research.
