There are many behaviors reflected in emotional and physiological reactions that can be studied by script-driven imagery paradigms. For instance, the design is suitable to investigate patterns of emotional and physiological response to trauma-related memory. We were particularly interested in verifying whether there is a distinct BPD subgroup mainly characterized by a dissociative reaction pattern.
In our study42, the assessments took place at the Department of Psychiatry and Psychotherapy I of the University of Ulm/Centre for Psychiatry Suedwuerttemberg. The recruitment was realized at the in-patient section 2056 of the headquarters Weissenau, Centre for Psychiatry Suedwuerttemberg. We recruited 28 participants with a clinical diagnosis of BPD. The BPD group was divided according to the established cutoff score of 1.5 of the PDEQ questionnaire for a peritraumatic dissociative reaction (low vs. high): BPD and PD (n = 15) and BPD only (n = 13). A control group of 15 persons with trauma histories, but without trauma-related or other psychological disorders was recruited from the staff of the Centre for Psychiatry Suedwuerttemberg.
Our study investigated differences between groups with regard to physiological and psychological measures. Among representative findings demonstrating the efficacy of the protocol, significant group differences resulted with respect to the HR differences between trauma-related scripts and scripts of everyday events (positive and neutral), due to a significant decrease of HR during memory of traumatic events in participants with BPD and a history of PD as compared to the BPD only group and controls (Figure 3). Yet, the analyses of SC responses did not show such differences.
Regarding self-report ratings, traumatic memories triggered for instance more dissociation than both positive and neutral memories (Figure 4). Besides, subjects with BPD and PD rated all memories as more dissociation provoking than other BPD participants and controls. The analyses of clinical data added valuable insight in the clinical profiles of BPD participants affected by severe PD responses who also showed a higher traumatic exposure, more severe symptoms and more comorbid disorders than the other BPD participants in Table 1. A multiple linear regression analysis to determine predictors of HR responses to trauma-related memory within the clinical sample indicated that PD level was the strongest predictor, followed by borderline symptom severity and level of dissociative experiences (Table 2).
Figure 1. Example of a personalized trauma-related script for the use within a script-driven experiment. Please click here to view a larger version of this figure.
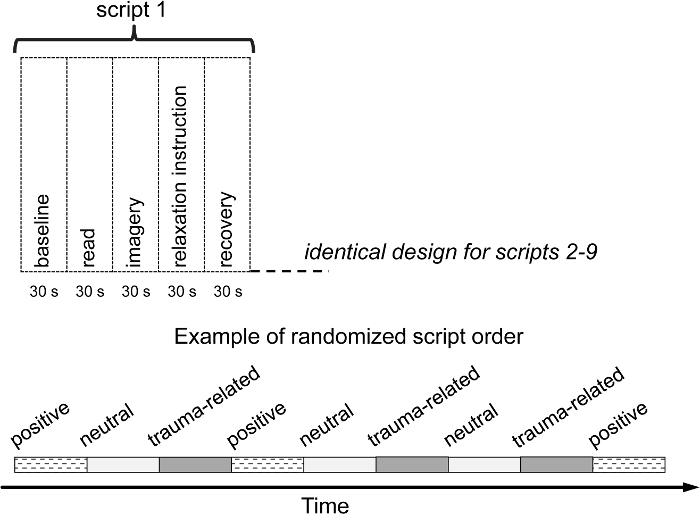
Figure 2. Graphic representation of the experimental design. Please click here to view a larger version of this figure.
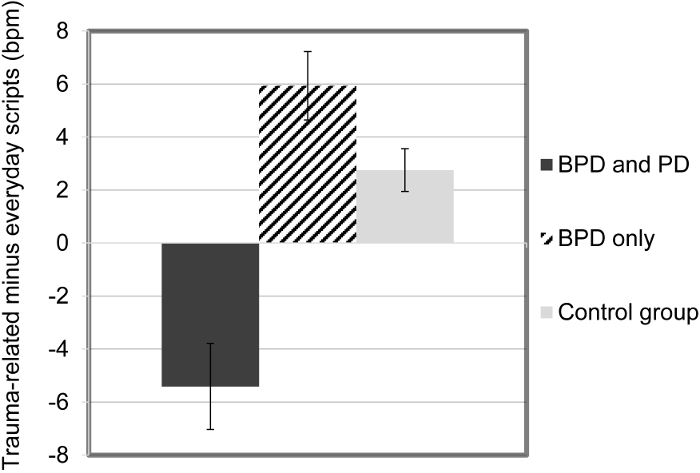
Figure 3. Means (and SE) of heart rate responses (difference score trauma-related minus everyday scripts) during memory of traumatic situations, by groups. This figure has been modified from the original figure [Bichescu-Burian et al.38], with permission from Psychophysiology. Please click here to view a larger version of this figure.
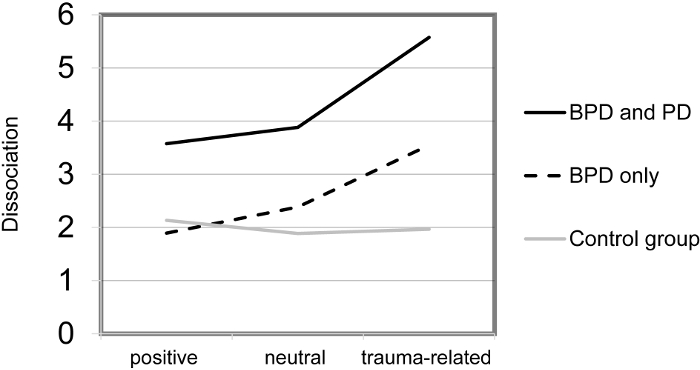
Figure 4. Means of self-rated levels of dissociation during memory of positive, neutral, and traumatic situations, by groups. This figure has been modified from the original figure [Bichescu-Burian et al.38], with permission from Psychophysiology. Please click here to view a larger version of this figure.
| (A) | ||||
| BPD and PD (n = 15) |
BPD only (n= 13) |
Control group (n =15) |
p | |
| Demographics | ||||
| Age, M (SD) | 25.53 (9.4) | 24.38 (8.8) | 23.87 (6.3) | n.s. |
| Education (years), M (SD) | 10.40 (1.2) | 10.54 (1.3) | 11.13 (1.1) | n.s. |
| Traumatic events | ||||
| CAPS event types, M (SD) | 7.40 (2.9)a | 6.08 (3.0) | 3.87 (2.3)a | < .01 |
| Rape/rape attempt (%) | 13 (86.7) | 8 (61.5) | 2 (13.3) | < .001 |
| CTQ score, M (SD) | 88.47 (28.0)a | 69.54 (18.5) b | 39.67 (10.4) a, b | < .001 |
| Emotional abuse (SD) | 18.27 (6.7)a | 14.62 (5.9)a, b | 7.67 (2.0)b | < .001 |
| Emotional neglect (SD) | 19.27 (5.3)a | 16.31 (4.4)a, b | 9.60 (4.1)b | < .001 |
| Physical abuse (SD) | 12.07 (6.0)a | 9.38 (6.1) | 5.53 (0.9)a | < .01 |
| Physical neglect (SD) | 12.60 (4.3)a | 10.23 (3.1)a, b | 5.50 (0.8)b | < .001 |
| Sexual abuse (SD) | 14.53 (8.3)a | 10.92 (7.1) | 6.67 (5.2)a | < .05 |
| Unpredictability (SD) | 11.07 (3.9)a, b | 8.08 (3.2)a, c | 4.33 (2.2)b. c | < .001 |
| PDEQ score (SD) | 2.71 (0.7)a, b | 1.21 (.2)a, b, c | 0.86 (0.6)c | < .001 |
| Clinical symptoms | ||||
| BSL score, M (SD) | 2.52 (0.8)a, b | 1.78 (0.7)a, c | 0.48 (0.4)b, c | < .001 |
| DES score, M (SD) | 34.66 (20.9)a, b | 15.91 (11.8)a | 4.90 (2.5)b | < .001 |
| SCL-14 score, M (SD) | 2.21 (0.9)a, b | 1.36 (.6)a, c | 0.18 (0.1)b, c | < .001 |
| Note. Significant differences between each pair of groups as revealed by post hoc comparisons are marked by identical characters. | ||||
| (B) | ||||
| BPD and PD (n = 15) |
BPD only (n = 13) |
p | ||
| Clinical symptoms | ||||
| CAPS score, M (SD) | 83.7 (28.0) | 58.5 (25.9) | < .05 | |
| GSI score of the SCL-90-R, M (SD) | 2.1 (0.7) | 1.3 (0.6) | < .01 | |
| Diagnoses | ||||
| PTSD, as diagnosed by CAPS (%) | 14 (93.3) | 7 (53.8) | < .05 | |
| Dissociative disorder, based on SCID-D (%) | 12 (80.0) | 1 (7.7) | < .001 | |
| Number of SCID-I diagnoses, M (SD) | 3.20 (1.5) | 1.77 (0.8) | < .01 | |
| Major depression disorder, by SCID-I (%) | 10 (66.7) | 5 (38.5) | n.s. | |
| Anxiety disorders, by SCID-I (%) | 8 (53.3) | 6 (46.2) | n.s. | |
| Substance use disorders, by SCID-I (%) | 9 (60.0) | 1 (7.7) | < .01 | |
| Eating disorders, by SCID-I (%) | 8 (53.3) | 2 (15.4) | < .05 | |
| Obsessive-compulsive disorders, by SCID-I (%) | 4 (26.7) | 1 (7.7) | n.s. | |
| Bipolar disorders, by SCID-I (%) | 1 (6.7) | 3 (23.1) | n.s. | |
| Adjustment disorders, by SCID-I (%) | 1 (6.7) | 2 (15.4) | n.s. | |
| Note. For continuous variables, t tests were calculated; for dichotomous variables, χ2 tests were applied. | ||||
Table 1. Clinical and other characteristics (A) of the three groups and (B) of the two clinical groups. This table was published in Bichescu-Burian et al.42, with permission from Psychophysiology.
| Model and significant predictor variables | R2 | df | p | B | SE | β | t | Partial regression p |
| Model 1 | .42 | 5 | < .01 | |||||
| PDEQ score | -5.81 | 1.96 | -.66 | -2.96 | < .01 | |||
| BSL score | -5.67 | 3.37 | -.60 | -1.68 | n.s. | |||
| DES score | -0.18 | 0.11 | -.47 | -1.66 | n.s. | |||
| SCL-90-R score | -0.12 | 3.60 | -.01 | -0.03 | n.s. | |||
| DSS-4 score | -0.05 | 0.75 | -.01 | -0.06 | n.s. | |||
| Model 2 | .45 | 4 | < .01 | |||||
| PDEQ score | -5.83 | 1.81 | -.66 | -3.22 | < .01 | |||
| BSL score | -5.75 | 2.23 | -.60 | -2.57 | < .05 | |||
| DES score | -0.18 | 0.10 | -.47 | -1.70 | n.s. | |||
| DSS-4 score | -0.04 | 0.73 | -.01 | -0.06 | n.s. | |||
| Model 3 | .48 | 3 | < .001 | |||||
| PDEQ score | -5.85 | 1.74 | -.66 | -3.36 | < .01 | |||
| BSL score | -5.77 | 2.15 | -.61 | -2.68 | < .05 | |||
| DES score | -0.18 | 0.10 | -.47 | -1.75 | n.s. |
Table 2. Linear regression analyses within the BPD Sample (N = 28) for factors of HR responses to Traumatic Imagery. This table was published in Bichescu-Burian et al.42, with permission from Psychophysiology.
