The following protocol and its validation study have been approved by the Ethics Committee of the University and University Hospital of Liège (reference 2017-297) and comply with the institution's guidelines on human research. All subjects (or their legal surrogates) who contributed to the elaboration and validation of the scale gave their written informed consent to participate. All personal data were processed according to the General Data Protection Regulation.
This scale has been developed with the aim to provide a comprehensive diagnostic assessment tool that would allow the examination of a large spectrum of patients with varying levels of consciousness. Like the CRS-R on which it is based, the SECONDs does not require specific inclusion or exclusion criteria to be administered. However, it has been validated in a population of patients with prolonged DoC, with predefined inclusion and exclusion criteria (see Representative Results).
1. The Simplified Evaluation of CONsciousness Disorders (SECONDs)
- Before starting the behavioral examination, adjust the lighting of the room to be adequate to perform the exam and ensure the patient is comfortably positioned with the four limbs exposed and the head oriented as straight as possible.
- Turn off any TV, radio, or other potentially distracting stimuli.
- Note any recent changes in medication in the patient's current treatment regimen, with particular attention to sedative and psychoactive drugs.
- Select a mirror of a minimum recommended 10 cm x 10 cm size for a square-shaped mirror or a 10 cm in diameter for a round-shaped one.
NOTE: Items should be administered sequentially from A to H: observation, command-following (score 6), communication (conditional, scores 7 and 8), visual pursuit (score 4), visual fixation (score 3), localization to pain (conditional, score 2), oriented behaviors (score 5) and arousal (scores 1 and 0). This sequence does not follow the scores of the items ordinally. This order was designed to optimize the allocation of the patient's attentional capacities and reduce administration duration. Communication and localization to pain are conditional items and must be administered only under certain conditions (see corresponding sections). The final score corresponds to the score of the highest succeeded item and directly reflects the diagnosis. An additional index score can be calculated to obtain a more accurate measure of the observed behaviors and allows following the evolution of the patient over time (see corresponding section).
2. Observation (A)
- Stimulation: at any time during the assessment, if no sustained eye-opening is observed or if the patients stops following commands for at least one minute, administer auditory (i.e., use patient's own name, clapping hands), tactile (i.e., CRS-R arousal facilitation protocol16), or noxious stimulation (i.e., pressure on fingernail bed) to arouse the patient.
- Observe the patient for one minute and report spontaneous behaviors.
NOTE: Pay attention to vocalizations, spontaneous movements of the four limbs, head, lips, or eyes, as well as spontaneous interactions with the environment. - During the entire assessment, promote eye-opening before testing each item if needed. Observe the patient and report the presence of eye-opening, either spontaneously or in response to stimulation, as well as the presence of self-oriented behaviors or behaviors oriented toward the environment. See sections 8 and 9 for detailed scoring guidelines of oriented behaviors and arousal.
NOTE: If eye-opening is not possible, oculomotor command-following, visual pursuit, and visual fixation (see sections 3, 5, 6) should be assessed by opening the patient's eyes manually. See section 9 (arousal) for detailed scoring criteria for eye-opening.
3. Command-following (B)
- Select three simple movements that were not observed as spontaneously repetitive during the observation period. Appropriate examples include: 'Move your hand', 'Turn your head', 'Blink twice', 'Look at [object or person]', 'Look up/down', 'Open/close your mouth', 'Stick out your tongue', 'Say a word/make a sound'. Adapt the selection of commands to the physical abilities of the patient. In cases of suspected LIS, relate at least one command to eye movements.
- Test each command in three trials, with a 10-second interval between trials. A command may be repeated once within the same trial to increase the patient's motivation. If the first two commands are successfully performed (3/3 trials for both commands with accurate responses), the third command does not have to be administered.
- In cases of known or suspected deafness, administer written commands. If the patient does not react to any of the oral commands, test at least one written command.
- Score "6" for command-following if the patient accurately responds to 2/3 trials for at least one command. To be scored, the response has to be clear and must appear within 10 seconds following the command prompt (and not spontaneously). All unclear, ambiguous responses or reflexive movements due to spasms or grasping must not be scored. Report the commands used on the scoring sheet, as well as the number of successful trials.
4. Communication (conditional) (C)
NOTE: Perform a communication test if at least two distinct responses to command are successfully performed (i.e., at least 2/3 for two commands) or if the patient can express a "yes" and a "no", either verbally, through gestures, eye movements or writing, spontaneously or not.
- If no verbal response can be produced, base the communication code on previously identified motor responses. Clearly explain the code to the patient before starting (e.g., thumbs-up for a "yes" and thumbs-down for a "no") and employ the most frequently used code for this patient, if any. The examiner can remind the code to be used to the patient before each question.
NOTE: It is necessary to use two distinct responses; the absence of movement cannot be used for a "yes" or a "no". - First ask 5 binary autobiographical questions – (1) 'Is your name [incorrect name]?' (2) 'Are you born in [correct birth year]?' (3) 'Is your name [correct name]?' (4) 'Are you born in [incorrect birth year]?' (5) 'Do you have children?'
- If the patient fails to correctly answer the autobiographical questions, ask the following binary situational questions: (1) 'Are we in [place: hospital, home or else]?' (2) 'Am I wearing a hat?' (3) 'Are we at the swimming pool?' (4) 'Am I touching your hand?' (Touch) (5) 'Am I touching your face?' (Do not touch).
- Score "7" for intentional communication if the patient responds to at least three out of five questions from one question set, regardless of accuracy. Score "8" for functional communication if the patient correctly responds to the five questions from one question set (either autobiographical or situational). Report the nature of the "yes/no" code, the modality (verbal, written) and the type (autobiographical, situational) of the questions used, the number of responses and the number of correct ones.
NOTE: Question sets must be considered separately, and correct answers from distinct question sets cannot be added up when scoring the item.
5. Visual pursuit (D)
- To assign a visual pursuit score, move silently around the bed while observing whether the patient's gaze spontaneously and clearly follows this movement during at least two seconds in two different directions.
- If a clear pursuit is not spontaneously observed, position the mirror about 30 cm in front of the patient's face.
- After confirming that the patient can see their reflection, move the mirror slowly from left to right (or right to left, depending on the initial position of the patient's eyes), right to the left, top to bottom, and bottom to top for at least four seconds per movement.
- Score a "4" for visual pursuit if an uninterrupted visual pursuit is observed in two different directions for at least two seconds. Report the number of observed pursuits on each axis, the type of stimulus used (spontaneous, mirror), and whether manual eye-opening was employed.
6. Visual fixation (E)
- To score visual fixation, enter the patient's field of view and observe whether the patient's gaze spontaneously fixates on the examiner for at least two seconds in two different visual quadrants by turning toward the examiner (performing a saccadic eye movement).
- If no clear and spontaneous visual fixations are observed, present the mirror about 30 cm away from the patient's face in all four quadrants of the patient's visual field, but not in the axis of their gaze, for at least four seconds per quadrant.
- Score a "3" for visual fixation if two fixations are observed, either spontaneously or induced by the mirror. A clear change of gaze orientation toward the mirror (or examiner) followed by a fixation of at least two seconds should be observed. Report the quadrants in which the patient showed the fixations, as well as the type of the stimulus used (spontaneous, mirror), and whether manual eye-opening was employed.
7. Localization to pain (conditional) (F)
NOTE: Test localization to pain only if the patient did not demonstrate command-following (score of 5 or below)
- Place a pen or pencil on the patient's fingernail bed for five seconds before instructing the patient to 'Remove your hand to avoid the pain'.
- If the patient does not remove the hand within the next five seconds, administer pressure on the nail bed with the pen or pencil for five seconds. One trial should be performed on each hand. If the patient removed the hand after the warning, do not apply pressure and directly proceed to the other hand and repeat the warning.
- Score "2" for localization to pain if, during at least one of the two trials, the non-stimulated hand of the patient clearly touches the stimulated hand. If the patient clearly removes the pain-stimulated hand after the warning but before the stimulation on both trials (anticipation response), score "6" for command-following. Report the side (L or R) of each observed localization and anticipation response (always report stimulated side).
8. Oriented behaviors (G)
- To assess oriented behaviors, perform continuous observation as described in 2.3. and score oriented behaviors by considering all of the behaviors observed during the entire examination. These behaviors may include (but are not limited to) scratching themselves, grabbing the bed sheets, holding the bed, pulling on the clothes/tracheostomy/gastrostomy/catheter, placing the hand on the mouth to cough, smiling/laughing/crying contextually, stereotyped verbal response or gesture when spoken to (e.g., grunt, head nod or thumbs up), or any other automatic non-reflexive behaviors.
NOTE: Yawning should not be scored as an automatic non-reflexive behavior. - Score "5" for oriented behaviors if the patient presents at least one clearly observed oriented behavior. Report the type and the number of times each behavior is observed.
9. Arousal (H)
- To assess arousal, perform continuous observation as described in 2.3. and score "0" for no arousal if, during the entire evaluation, the patient never opened the eyes, with or without stimulation (including nociceptive stimulation). Score "1" for arousal if the patient opened the eyes at least once during the assessment, either spontaneously or following stimulation. Report the approximate percentage of time the eyes were open throughout the examination (0-25%; 25-50%; 50-75%; 75-100%).
- Specify if the eye-opening happened spontaneously or following a noxious, tactile, or auditory stimulation, as well as the number of stimulations of each type that were administered.
10. Additional index
NOTE: An additional index score has been developed to give a more accurate account of the behaviors observed during the assessment, allowing monitoring of a patient's level of consciousness over time. For each successful item, specific index points correspond to the type of behavior observed (see Table 1).
- Calculate the additional index score by adding up the points earned in each item tested during the assessment. This measure ranging from 0 to 100 is independent from the final score and diagnosis but is designed to more precisely follow the evolution of a patient who may exhibit subtle clinical changes without modification of the diagnosis across repeated assessments.
| Diagnosis | Score | Item | Sub-item | Additional index points |
| EMCS | 8 | Communication* | 5 answers (accurate) | 29 |
| MCS+ | 7 | 3 or 4 answers (accurate) | 21 | |
| 5 answers (inaccurate OK) | 14 | |||
| 3 or 4 answers (inaccurate OK) | 7 | |||
| 6 | Command-following | 2 commands 3/3 | 24 | |
| 2 commands 2/3 | 18 | |||
| 1 command 3/3 | 12 | |||
| 1 command 2/3 | 6 | |||
| MCS- | 5 | Oriented behaviors | More than two different movements | 15 |
| Two different movements | 10 | |||
| One movement | 5 | |||
| 4 | Visual pursuit | On four (all) occasions | 16 | |
| On three occasions | 12 | |||
| On two occasions | 8 | |||
| 3 | Visual fixation | On four (all) occasions | 12 | |
| On three occasions | 9 | |||
| On two occasions | 6 | |||
| 2 | Pain localization* | On both hands | 4 | |
| On one hand | 2 | |||
| UWS | 1 | Arousal | Spontaneously | 4 |
| To auditory stimulation | 3 | |||
| To tactile stimulation | 2 | |||
| To pain | 1 | |||
| Coma | 0 | None | 0 |
Table 1. Scoring, associated diagnosis, and additional index points. Additional index points obtained for each conditional item should be added to calculate the additional index score, ranging from 0 to 100. Zero additional index point should be scored for non-administered conditional items (e.g., pain localization when command-following is present) or unsuccessful items (i.e., when the criteria to score the item are not met). * denotes conditional items.
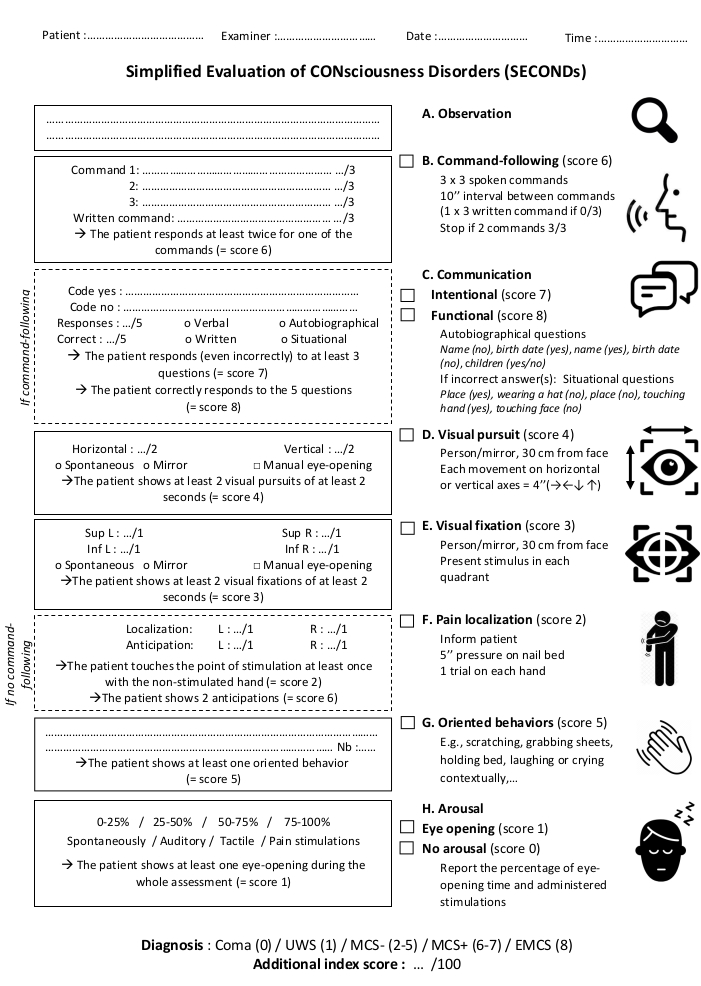
Figure 1. Administration protocol of the SECONDs. The scale features eight items (six mandatory – A, B, D, E, G, H and two conditional – C, F) presented in the order of administration. All required fields should be completed and the highest score used to determine the patient's behavioral diagnosis. Please click here to view a larger version of this figure.
Figure 1 presents the administration protocol and scoring sheet of the SECONDs. In a previous French validation study performed on 57 DoC patients22, the inclusion criteria included the presence of severe acquired brain injury, a prolonged DoC (i.e., at least 28 days since injury), minimum age of 18 years, no history of neurological or psychiatric deficit, oral fluency in French, and a stable medical condition. Three SECONDs and one CRS-R assessments were performed on two consecutive days, including randomization and blinding procedures. The administration duration of the SECONDs (median = 7 min; interquartile range = 5-9 min) was significantly shorter compared to the CRS-R (median = 17 min; interquartile range = 12-22 min; W = 8791, p < 0.001). The concurrent validity was excellent for the CRS-R and the SECONDs' best diagnosis (KW = 0.85). The intra-rater reliability (KW = 0.85) and inter-rater reliability (KW = 0.85) were also excellent. The CRS-R total score correlated with the score of the best SECONDs (rs = 0.92; S = 2343.8, p<0.001).The diagnostic disagreement between the best SECONDs and the CRS-R was 11/57 (19%) (Table 2). There was a significant negative correlation between the SECONDs administration duration and the patient level of consciousness (Spearman's rho = -0.49, p = 2.26 x10-12, S = 1.40E6). Shorter assessments corresponded to patients with better diagnoses (median administration duration = 8 min for UWS patients, 7 min for MCS patients, 5 min for EMCS patients). These data tend to rule out the possibility that a longer assessment time may have increased the chance to observe conscious behaviors.
| CRS-R | Same-day SECONDs | Best SECONDs | |
| Administration duration | Median = 17 min, IQR = 12-22 min | Median = 7 min, IQR = 5-9 min | |
| W = 8791; p < 0.001 | |||
| Diagnosis | |||
| UWS patients | 12 | 14 | 13 |
| MCS patients | 28 | 27 | 25 |
| EMCS patients | 17 | 16 | 19 |
| Concurrent validity with the CRS-R | KW = 0.79; 48/57; 84.21% | KW = 0.84; 50/57; 87.72% | |
| Intra-rater reliability | KW = 0.91; 53/57; 92.98% | ||
| Inter-rater reliability | KW = 0.82; 49/57; 85.96% | ||
| Correlation between SECONDs and CRS-R total scores | rs = 0.91 | rs = 0.92 | |
| S = 3110.2; p < 0.001 | S = 2343.8; p < 0.001 | ||
Table 2. Representative results from the SECONDs validation study22. Diagnostic assessments of patients with disorders of consciousness were compared, using either the Coma Recovery Scale - Revised (CRS-R - left column), the Simplified Evaluation of CONsciousness Disorders (SECONDs) performed on the same day as the CRS-R (middle column) or the SECONDs with the best diagnosis (right column). Administration durations were compared using a Mann Whitney U test (IQR = interquartile range; W = Mann-Whitney test statistic). Concurrent validity, intra-rater reliability and inter-rater reliability were calculated using Fleiss' weighted coefficients (KW). Spearman's rank correlation coefficients (rs) were computed to compare total scores of the SECONDs and the CRS-R (S = Spearman's test statistic).
To highlight the importance of a meticulous administration procedure and the need to follow the scoring guidelines thoroughly, three fictional illustrative cases are presented featuring frequent pitfalls that may be encountered while administering this scale (Figure 2). These examples are based on realistic clinical situations and aim to demonstrate how a single small deviation in the administration procedure can result in a misdiagnosis and, consequently, in inappropriate patient management. As a general rule, examiners should always attempt to elicit the best possible response for a given item (e.g., by promoting arousal, encouraging the patient, and optimizing the testing environment) but should score responses that are clear, unequivocal, and reproducible only. Any ambiguous or questionable responses should not be scored but can be mentioned as a comment and re-evaluated in future assessments.
Case 1 illustrates the importance of command selection. An examiner is called in to evaluate a 34-year-old female patient diagnosed in UWS for several years who has begun presenting blinking, agitation, tongue protrusion, and upward eye movements since the morning. The nurse asks whether the patient could suffer from a LIS and is worried that the patient may be trying to communicate and that the patient has been conscious the whole time. The patient has been given domperidone during the night because of nausea and vomiting. Upon arrival to the room, the patient can be observed to exhibit repeated episodes of sustained upward gaze lasting around 10 seconds each. When administering the SECONDs, no response is obtained to the commands 'Move your hand', 'Open your mouth' or 'Look down'. The patient exhibits no visual pursuit or fixation, no localization to pain, and no oriented behaviors. Selection of the 'Look up' command could have fortuitously resulted in a score of 6 and therefore an erroneous diagnosis of MCS+, as spontaneous repeated movements must not be used to test command-following. A correct administration of the SECONDs following the guidelines results in a score of 1 and a diagnosis of UWS. This patient is suffering from an oculogyric crisis triggered by the administration of domperidone, with typical episodes of involuntary upward bilateral elevation of the eyes.
Case 2 illustrates the importance of question selection when testing communication. A 67-year-old female patient is admitted to the emergency room hospital for acute ethanol consumption with respiratory failure. Now medically stable, the patient's level of consciousness must be assessed. The patient correctly responds to commands ('Squeeze my hand', 'Look up') with some delay. When communication is tested using autobiographical questions, the patient provides 5/5 verbal responses but only 2/5 are correct. When testing communication using the situational questions, the patient answers with 5/5 correct answers. This patient suffers from Korsakoff syndrome associated with retrograde amnesia due to chronic alcohol consumption and thiamine deficiency. Testing communication using only autobiographical questions would result in a score of 7 and a diagnosis of MCS+, due to memory deficits and not altered consciousness. Correct administration of the SECONDs testing communication with both question sets would result in a correct score of 8 and a diagnosis of EMCS.
Case 3 illustrates the importance of manual eye-opening. A 50-year-old male patient is admitted to the intensive care unit for a respiratory failure due to envenomation from a cobra snake bite. He is now medically stable and his level of consciousness must be assessed, as the medical staff says the patient does not open his eyes even after withdrawal of all sedative drugs. Upon administration of the SECONDs, an absence of eye-opening despite auditory, tactile, and noxious stimulation is observed. No movement of the limbs can be observed either spontaneously or when testing command-following. However, when manually opening the eyelids, the patient shows command-following and functional communication using eye movements ('Look up for yes' and 'Look down for no'). This patient has bilateral neurotoxic ptosis and limb paralysis due to the neurotoxins contained within the venom but is fully conscious. Administration of the SECONDs without manual eye-opening would have resulted in a score of 0, corresponding to a diagnosis of coma, while a correct administration reveals a score of 8, which describes an emergence of the minimally conscious state.
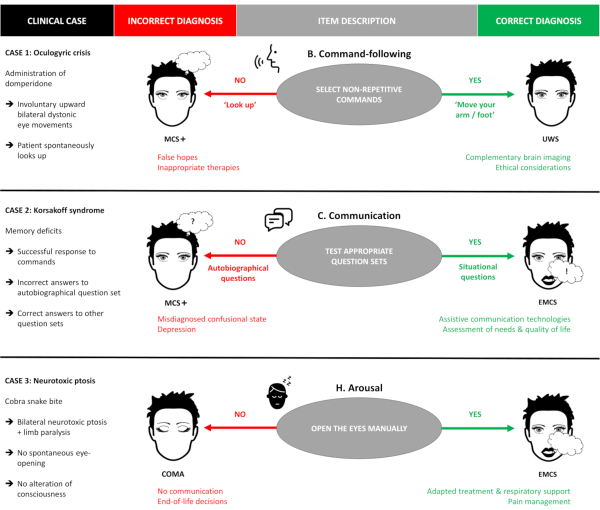
Figure 2. Illustrative clinical cases. Three fictional clinical cases illustrating frequent administration pitfalls of the SECONDs are presented. The red column indicates the potential outcomes resulting from a suboptimal administration of the scale, while the green column describes the potential outcomes resulting from a correct administration of the SECONDs following the guidelines (e.g., in case 1, the patient is misdiagnosed as MCS+ if spontaneously repetitive commands are tested, and correctly diagnosed as UWS if appropriate non-repetitive commands are used). MCS+: minimally conscious state plus; UWS: unresponsive wakefulness syndrome; EMCS: emergence of the minimally conscious state. Please click here to view a larger version of this figure.
