Twelve pigs underwent coronary artery occlusion followed by 12 min of ventricular fibrillation and 5 min of CPR. Eight pigs were successfully resuscitated, and seven survived at 96 h post AMI-cardiac arrest-ROSC. All echocardiographic variables at different time-points during the study are summarized in Table 1.
Changes in heart rate (HR) and systolic echocardiographic parameters
HR increased significantly at 2 h and 4 h post-AMI-cardiac arrest-ROSC compared with baseline (BL) (mean ± SEM: +64 ± 9 and +56 ± 12 bpm, p < 0.001 and p < 0.01, respectively) together with ESV (+15 ± 3 and +18 ± 4 mL, p < 0.01 for both), while EDV did not change significantly at the different times. The mean differences in LVEF between BL and 2 h and 4 h were -40 ± 4.1 and -39 ± 4.0 absolute points %, respectively (p < 0.001 for both) (Figure 4).
From 2 h to 96 h post AMI-cardiac arrest-ROSC, HR tended to normalize, (mean ± SEM difference -49 ± 9.1 bpm, p < 0.05). LVEF improved, rising 24.9 ± 2.5 points percent (p < 0.05), but it remained below BL. Changes in LV volumes were minimal and not significant; results were similar for changes between 4 h and 96 h post-AMI-cardiac arrest-ROSC (Figure 4 and Figure 5).
Changes in diastolic echocardiographic parameters
DT was the only echocardiographic diastolic variable that changed significantly at the different study time-points (Figure 6). At 2 h, DT decreased 16% from BL and maintained the decrease at 4 h post AMI-cardiac arrest-ROSC. At 96 h post AMI-cardiac arrest-ROSC, DT returned similar to those at BL.
LV regional motility 96 h post AMI-cardiac arrest-ROSC
The mean ± SEM number of akinetic/dyskinetic (A/D) segments was 4.2 ± 0.7 and WMSI was 26 ± 4.4%. The most frequently compromised segments were mid anterolateral, mid-inferoseptal, apical anterior, and apical inferior.
Table 1: Echocardiographic variables at different times after AMI-cardiac arrest-ROSC. BL, baseline; HR, heart rate; AoD, aortic diameter; LAD, left atrium diameter; AWThd, diastolic anterior wall thickness; AWThs, systolic anterior wall thickness; EDD, end-diastolic diameter; ESD, end-systolic diameter; IPWThd, diastolic infero-posterior wall thickness; IPWThs, systolic infero-posterior wall thickness; SF, shortening fraction; EDV, end-diastolic volume; ESV, end-systolic volume; LVEF, left ventricle ejection fraction; E vel, peak mitral inflow E velocity; A vel, peak mitral inflow A velocity; DT, deceleration time; CO, cardiac output; SV, stroke volume; s' sept, TDI-derived mitral annular s' septal velocity; e' vel, TDI-derived mitral annular e' septal velocity; a' vel, TDI-derived mitral annular a' septal velocity; s' lat, TDI-derived mitral annular s' lateral velocity; e' lat, TDI-derived mitral annular e' lateral velocity; a' lat, TDI-derived mitral annular a' lateral velocity; E/e' septal ratio, peak mitral inflow velocity (E vel) to TDI-derived mitral annular e' septal velocity ratio; E/e' lateral ratio, peak mitral inflow velocity (E vel) to TDI-derived mitral annular e' lateral velocity ratio. Data are mean ± SEM. Please click here to download this Table.
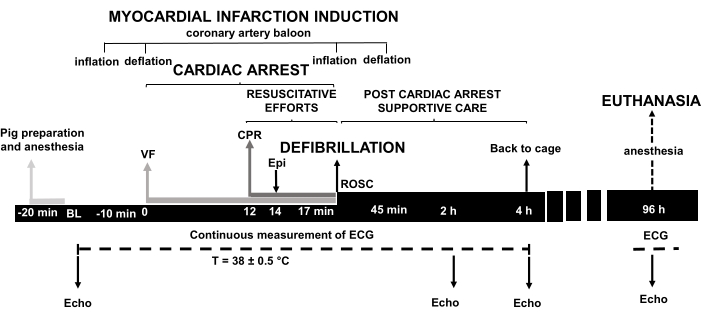
Figure 1: Experimental model of cardiac arrest. VF, ventricular fibrillation; CPR, cardiopulmonary resuscitation; Epi, epinephrine; ROSC, return of spontaneous circulation; BL, baseline; ECG, electrocardiogram; Echo, echocardiography; h, hours; min, minutes. Please click here to view a larger version of this figure.
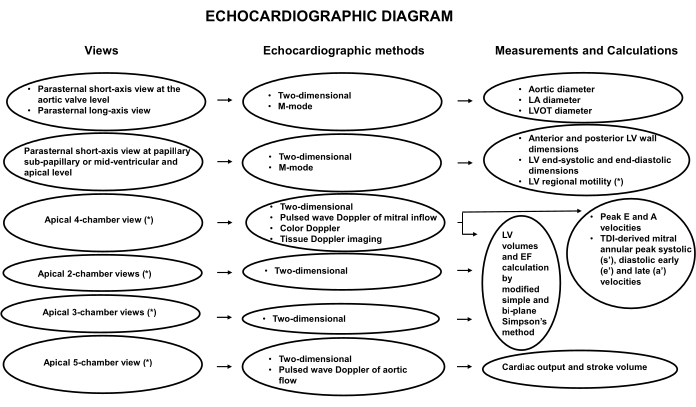
Figure 2: TTE flow-chart in a pig model of ischemic cardiac arrest. LA, left atrium; M-mode, mono-dimensional; LV, left ventricle; LVOT, left ventricle outflow tract; LVEF, left ventricular ejection fraction; PW, pulsed-wave; TDI, tissue Doppler imaging. Please click here to view a larger version of this figure.
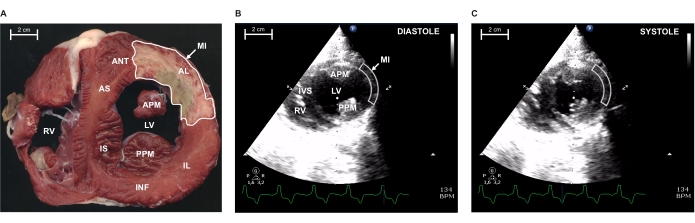
Figure 3: Myocardial infarction (MI) extension at papillary level by morphometry and bi-dimensional echocardiography 96 h after coronary artery occlusion. (A) Representative ex vivo 0.5 cm slice of pig heart at the papillary level, stained with triphenyl tetrazolium chloride (TTC) to display the healthy myocardial zone (red) against the infarcted one (brown). Echocardiographic 2D-parasternal short-axis view at the papillary level in diastole (B) and in systole (C). Arrows indicate the delimited MI areas indicated in A, B, and C. RV, right ventricle; IS, infero-septal wall; AS, antero-septal wall; IVS, intraventricular septum; APM, anterior papillary muscle; PPM, posterior papillary muscle; LV, left ventricle; AL, antero-lateral wall; ANT, anterior wall; INF, inferior wall; IL, infero-lateral wall. Please click here to view a larger version of this figure.
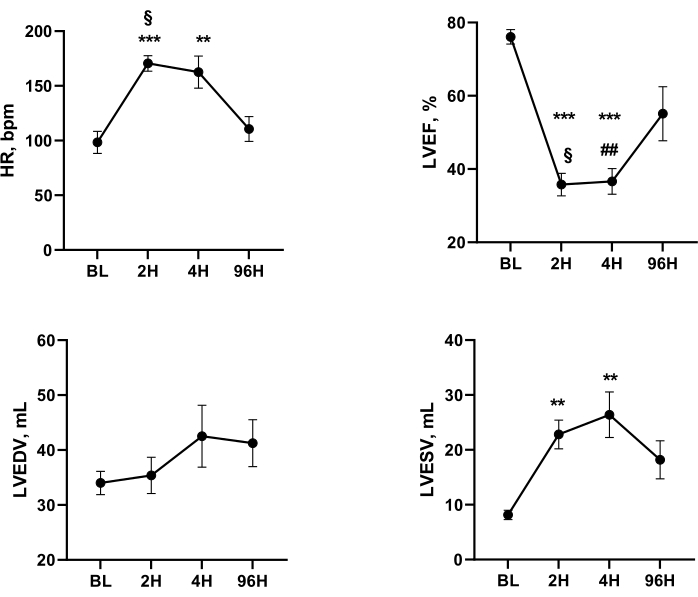
Figure 4: Systolic function parameters with heart rate at BL and after AMI, cardiac arrest, and resuscitation. One-way ANOVA for repeated measurements and Tukey's post-hoc test: *** p < 0.001, ** p < 0.01 vs BL; § p < 0.05 2 h vs 96 h; # p < 0.05, ## p < 0.01 4 h vs 96 h. BL, baseline; 2H, 2 h after AMI-cardiac arrest-ROSC; 4H, 4 h AMI- cardiac arrest-ROSC; 96H, 96 h AMI- cardiac arrest -ROSC; HR, heart rate; LVEF, left ventricular ejection fraction; LVEDV, left ventricular end-diastolic volume; LVESV, left ventricular end-systolic volume. Please click here to view a larger version of this figure.
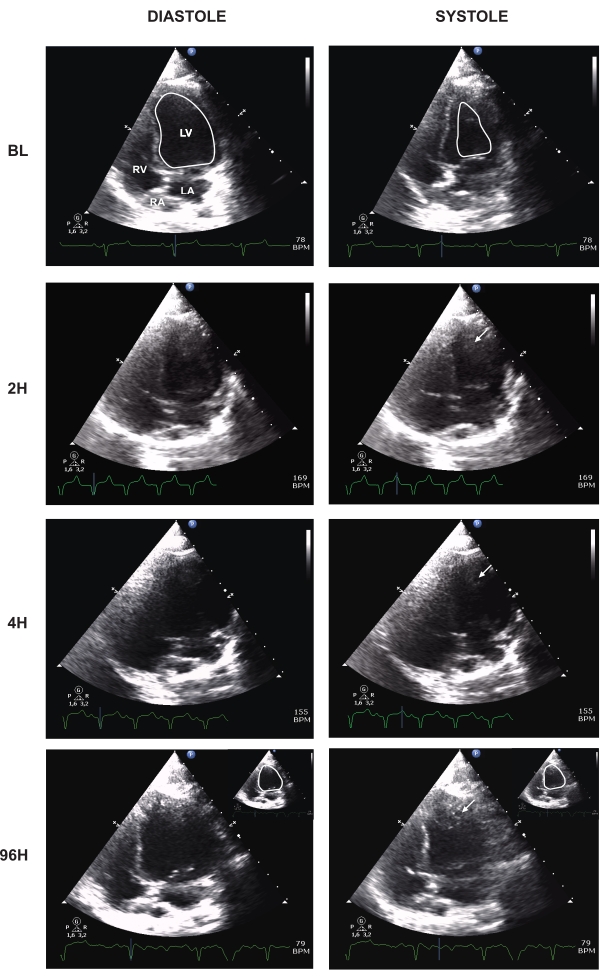
Figure 5: Apical four-chamber view at different times after AMI-cardiac arrest-ROSC. BL, baseline; H, hour; LV, left ventricle; RV, right ventricle; LA, left atrium; RA, right atrium. Arrows indicate apical thrombi near akinetic segments. Baseline and 96 h LV systolic and diastolic internal borders are shown in white. Please click here to view a larger version of this figure.
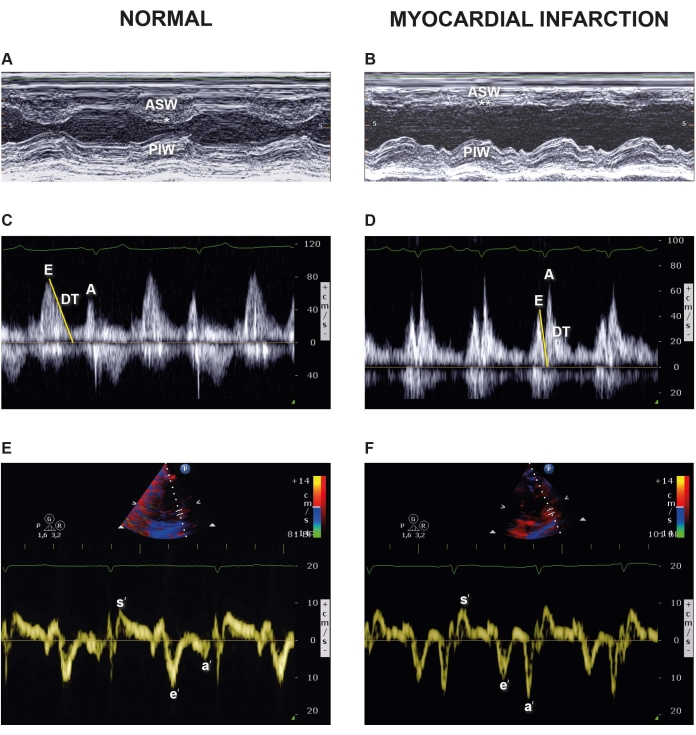
Figure 6: M-mode traces of short axis, MV color Doppler and TDI images in a healthy pig and 96 h after myocardial infarction (MI)-cardiac arrest-ROSC. Representative images of the LV from M-mode echocardiography at baseline (A) and 96 h after AMI-cardiac arrest-ROSC (B). ASW, anteroseptal wall; PIW, posteroinferior wall. * = normo-kinetic; ** = severely hypokinetic. Apical four-chamber view: pulse wave Doppler (PW) of the trans-mitral valve flow at baseline (C) and 96h after AMI-cardiac arrest-ROSC (D). Evel, PW early peak mitral inflow velocity; Avel, PW late peak mitral inflow velocity; DT, deceleration time. Representative images of septal and lateral TDI velocities at baseline (E) and (F) 96 h after MI-cardiac arrest-ROSC. s', TDI systolic velocity; e' TDI early diastolic velocity; a', TDI late diastolic velocity. Please click here to view a larger version of this figure.
