The described approach to induce ALI in mice was validated by assessing cytokine expression, neutrophil granulocyte infiltration, and alveolo-capillary barrier disruption 24 h and 72 h after LPS instillation. PBS-injected animals served as control. Intratracheal LPS administration induced a robust pulmonary proinflammatory response. Expression of TNF-α in lung tissue was significantly upregulated, reaching a sustained and more than 50-fold increase compared to the control animals [RQ (TNF-α/18s); 24 h: 53.7 (SD = 11.6); 72 h: 55.0 (SD = 20.6); p < 0.05)] (Figure 3A). Leukocyte invasion into tissue and alveolar space is a hallmark and characteristic for the development of ALI13. FACS analysis revealed a significant infiltration of neutrophil granulocytes (NG) into the lung interstitium, with absolute cell count having increased almost 9-fold compared to the controls after 24 h [65,243 (SD = 15,855) vs. 7,358 (SD = 4,794), p < 0.05] (Figure 3B). Absolute NG count slightly decreased after 72 h; however, the factor increases compared to the controls remained stable [48,946 (SD = 5,223) vs. 5,510 (SD = 654), p < 0.05]. Consistent with interstitial NG infiltration, MMP-9 expression in whole lung tissue was likewise significantly increased over the total observation period [RQ (MMP-9/18s), 24 h: 7.4 (SD = 1.5); 72 h: 10.4 (SD = 2.0); p < 0.05] (Figure 3C).
NG were not only increased in the lung tissue but also in the BAL fluid. The fold increase compared to control animals was more pronounced than in lung tissue, with absolute NG counts 24 h following ALI induction of 52,005 (SD = 21,906) vs. 1,829 (SD = 1,724) (p < 0.05) (Figure 3D). After 72 h, NG were increased to 37,254 (SD = 4,478) vs. 17.0 (SD = 10.8) (p < 0.05). Lung edema due to severe impairment of the alveolo-capillary barrier is pathognomonic for the development of ALI, with LPS rapidly inducing endothelial apoptosis and increased permeability14,15. Analysis of albumin content in BAL fluid by ELISA revealed a significant loss of barrier function. 24 h following LPS instillation, albumin in BAL fluid was 43 ng/mL (SD = 13), compared to 20 ng/mL (SD = 9) under control conditions (p < 0.05) (Figure 3E). After 72 h, in ALI animals, albumin content was 48 ng/mL (SD = 14), compared to 29 ng/mL (SD = 9) (p < 0.05).
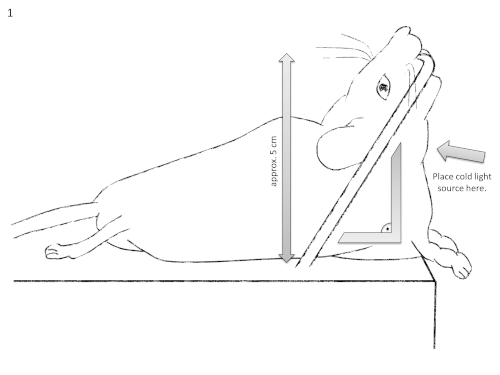
Figure 1: Schematic diagram of the intubation setting. It should be noted that the mouse's neck should be super-extended at a 90° angle relative to the operation table. Please click here to view a larger version of this figure.
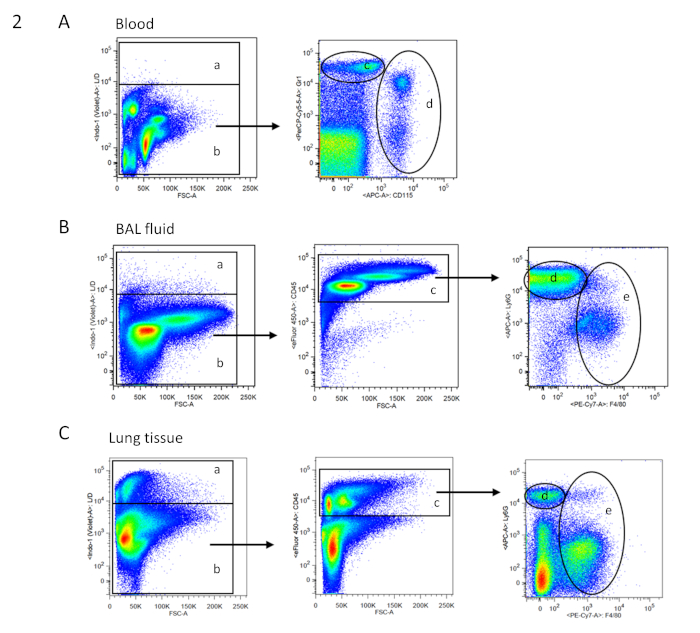
Figure 2: FACS gating strategy for blood, BAL, and tissue cells. Exemplary dot blots of FACS analysis are shown in two-parameter (dual color fluorescence) pseudocolor plots. Gating strategy for the respective samples is based on single cells. (A) Gating tree for blood cells: a = dead cells; b = living cells (according to live/dead cell staining; no CD45 staining necessary as in the blood, high autofluorescence makes the cell populations clearly distinguishable); d = neutrophil granulocytes; e = monocytes (according to Gr1 and CD115 staining). (B) Gating tree for bronchoalveolar lavage (BAL) fluid: a = dead cells; b = living cells (according to live/dead cell staining); c = CD45+ immune cells; d = neutrophil granulocytes; and e = macrophages (according to Ly6G and F4/80 staining). (C) Gating tree for lung tissue: a = dead cells; b = living cells (according to live/dead cell staining); c = CD45+ immune cells; d = neutrophil granulocytes; and e = macrophages (according to Ly6G and F4/80 staining). Please click here to view a larger version of this figure.
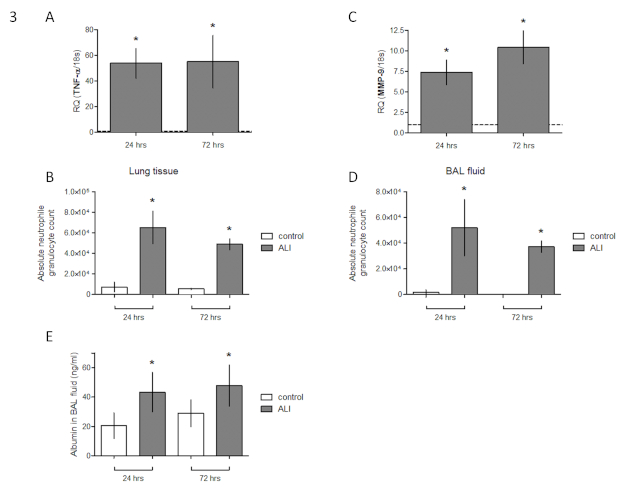
Figure 3: Validation of murine ALI model against control animals. (A) Expression of TNF-α in lung tissue of female C57BL/6 mice 24 h and 72 h following intratracheal LPS instillation (fold change of expression of sham operated animals). (B) FACS analysis of absolute neutrophil granulocyte count in lung tissue. (C) Expression of MMP-9 in lung tissue (fold change of expression of sham operated animals). (D) FACS analysis of absolute neutrophil granulocyte count in bronchoalveolar lavage fluid. (E) Albumin content in BAL fluid [mean ± SD, n = 7, Mann-Whitney U test, *p < 0.05 (vs. PBS control)]. This figure has been modified from Ehrentraut et al.8. Please click here to view a larger version of this figure.
| Name of Material/ Equipment | Volume (mL) |
| Dulbecco's Phosphate Buffered Saline (PBS), without calcium chloride and magnesium chloride, sterile | 1000 |
| Fetal calf serum (FCS) | 1 |
| Ethylenediaminetetraacetic acid (EDTA) solution | 1 |
| Sodium azide (NaN3) | 0.1 |
Table 1: Composition of FACS buffer.
| Name of Material/ Equipment | Suggested dilution | Mastermix for 10 samples: add to 200 µl FACS buffer (= 20 µl per sample): |
| Anti-CD115 (c-fms) APC | 0.5 µL/100 µL | 5 µL |
| Anti-CD11b (M1/70) – FITC | 0.5 µL/100 µL | 5 µL |
| Anti-CD45 (30-F11) – eF450 | 0.5 µL/100 µL | 5 µL |
| Anti-F4/80 (BM-8) – PE Cy7 | 0.5 µL/100 µL | 5 µL |
| Anti-Gr1 (RB6-8C5) | 0.5 µL/100 µL | 5 µL |
| Anti-Ly6C (HK1.4) PerCP-Cy5.5 | 0.5 µL/100 µL | 5 µL |
| Anti-Ly6G (1A8) APC/Cy7 | 0.5 µL/100 µL | 5 µL |
Table 2: Preparation of master mix for FACS staining. The table describes master mix preparation for 10 samples.
