Myh11-Cre/ERT2 R26R-EYFP Apoe-/- mice were injected with tamoxifen between six and eight weeks of age before being fed a high fat diet. At 18 weeks of high fat diet feeding, two groups of eight mice were treated weekly with either a mouse monoclonal anti-IL-1β antibody or an isotype-matched IgG control at 10 mg/kg for 8 weeks (Figure 1)7. Mice were sacrificed and perfused with a 4% PFA-PBS solution. Brachiocephalic arteries were dissected, processed, and sectioned as described above (Figure 2 and Figure 3).
After immunofluorescent staining with antibodies targeting the lineage tracing reporter (YFP) and phenotypic markers (ACTA2, LGALS3, RUNX2), a thickness of 8-10 µm of the BCA cross sections was imaged using a confocal microscope. Images of each individual staining, DAPI (nuclear staining), and DIC were acquired. Delineation of regions of interest for single cell counting (lesion, fibrous cap) was performed using DIC images (Figure 4). Single cell counting to determine the abundance of different SMC-derived populations was performed using ImageJ (Figure 5).
We present two representative immunofluorescent staining and single counting assessing the effect of IL-1β inhibition on cellular composition in advanced atherosclerotic lesions. First, staining was done for the SMC lineage tracing reporter YFP, the SMC marker ACTA2, and the macrophage marker LGALS3 in cross sections at two different locations of the BCA (480 µm and 780 µm from the aortic arch) (Figure 6). Single cell counting analysis in the fibrous cap region of these cross section were performed, and remarkable differences were found in the cellular composition of the fibrous cap area between mice treated with the anti-IL-1β antibody and mice treated with the isotype-matched IgG control (Figure 6A). Inhibition of IL-1β was associated with a decrease in YFP+ SMC and an increase in LGALS3+ cells (Figure 6B). Regarding the phenotypes of SMC populations, a decrease in the number of YFP+ACTA2+ SMC was observed, whereas the relative number of SMC-derived macrophages (YFP+LGALS3+) was significantly increased at both BCA locations (Figure 6C).
Finally, we investigated the effect of IL-1β inhibition on the SMC phenotypic transition into chondrogenic cells. This phenotypic transition is an important driver of vascular calcification, major feature of late-stage atherosclerosis14,32,33. BCA cross-sections were stained for the SMC lineage tracing reporter YFP, the osteochondrogenic marker RUNX2, and the macrophage marker LGALS3 (Figure 7A). The abundance and the origin of the RUNX2+ chondrogenic cells were characterized within the lesion area in our two experimental groups. We found that inhibition of IL-1β did not impact the overall number of RUNX2+ cells within the lesion, nor the proportion of SMC-derived (YFP+RUNX2+) and macrophage-derived (YFP-LGALS3+RUNX2+) chondrogenic cells (Figure 7B).
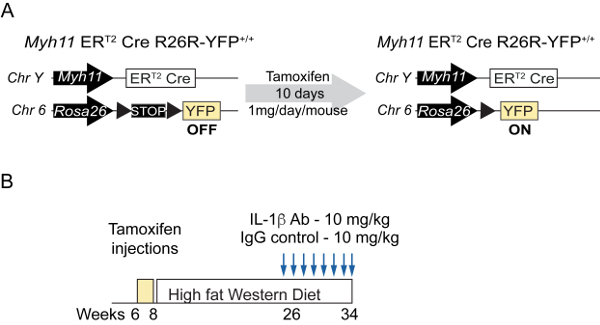
Figure 1: Intervention studies in Smooth Muscle cell lineage tracing mice. (A) Schematic representation of the Myh11-Cre/ERT2 R26R-EYFP Apoe-/- tamoxifen-inducible SMC specific lineage tracing mouse model. Treatment with tamoxifen induces recombination of the R26R-YFP locus and the excision of a STOP codon and the permanent expression of YFP by SMC. (B) Schematic of intervention studies in which Myh11-Cre/ERT2 R26R-EYFP Apoe-/- mice fed a Western diet for 18 weeks were injected weekly with the IL-1β antibody or an isotype-matched IgG control antibody at a concentration of 10 mg/kg for 8 weeks. Please click here to view a larger version of this figure.
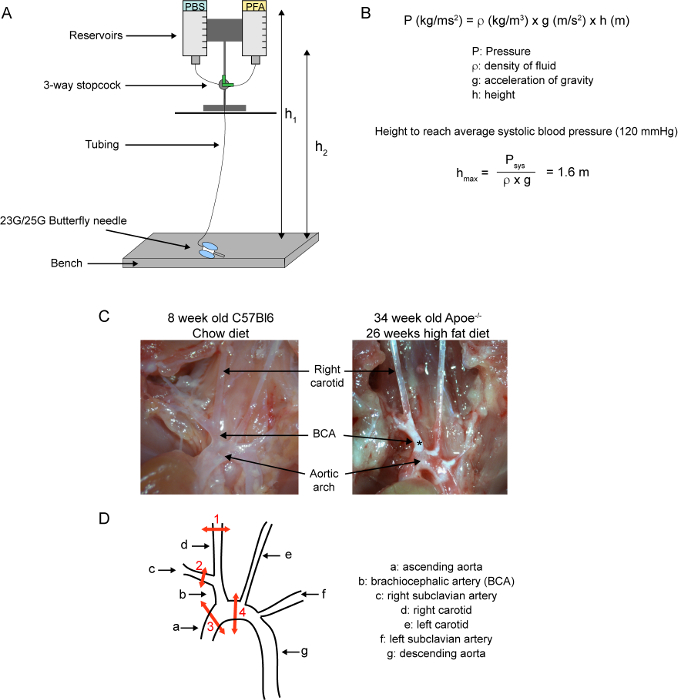
Figure 2: Brachiocephalic artery dissection. (A) Schematic of a gravity driven perfusion system. The system is set up at a precise height allowing perfusion at a pressure close to the average systolic blood pressure in mice. The pressure slightly varies with volume height as liquid is used during perfusion between height h1 and h2. (B) Equation for calculation of the pressure of static fluids and determination of the height to reach a pressure of perfusion equal to the C57Bl6 mouse average systolic blood pressure. (C) Pictures of the proximal aorta and branching arteries in C57Bl6 mouse fed a chow diet (left picture) and Apoe-/- mouse fed a high fat diet for 26 weeks (right picture). The asterisk indicates the presence of atherosclerotic lesions. (D) Schematic of the proximal aorta and branching arteries. Red arrows represent cuts for isolation of the right carotid and brachiocephalic artery isolation and numbers indicate the order of the cuts. Please click here to view a larger version of this figure.
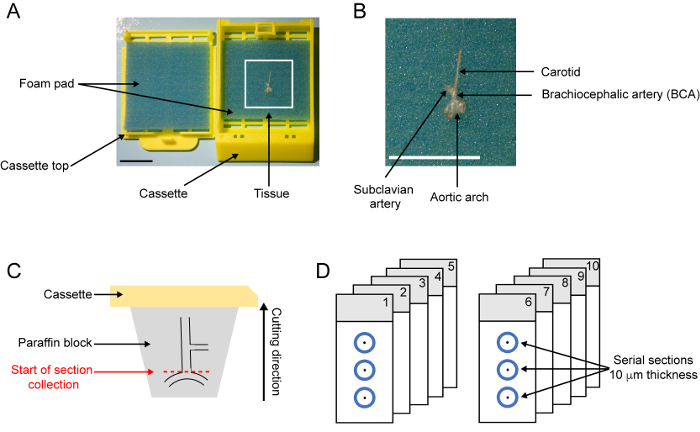
Figure 3: Tissue processing, embedding, and sectioning. (A) Photograph of an embedding cassette with BCA tissue. The BCA is positioned on a foam pad. (B) Zoom-in of the BCA positioned on the foam pad. The BCA is oriented with the aortic arch close to the label part of the cassette and the carotid straightened vertically. Scale bar: 1 cm. (C) Schematic of paraffin block after embedding of the brachiocephalic artery. (D) Schematic of serial slides with 10 µm-thick serial sections with indication of the distance from the aortic arch. Please click here to view a larger version of this figure.
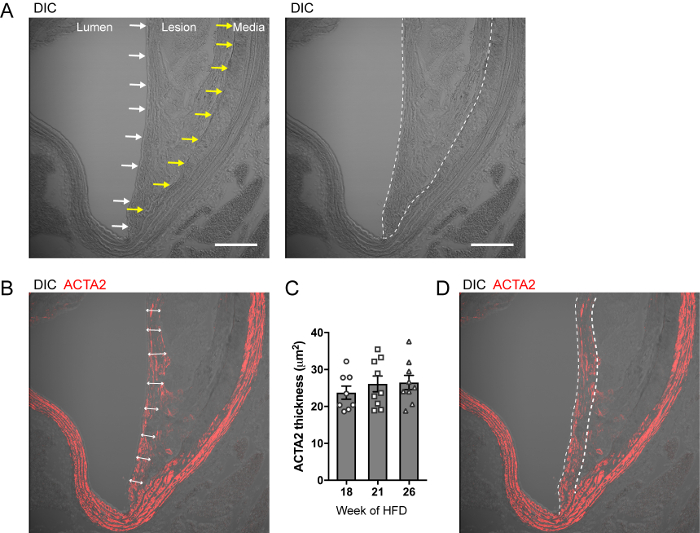
Figure 4: Delineation of the atherosclerotic lesion and fibrous cap area. (A) Representative micrographs of DIC image atherosclerotic lesion in brachiocephalic artery cross-sections from Myh11-Cre/ERT2 R26R-EYFP Apoe-/-. The luminal and the internal elastic lamina borders are localized by white and yellow arrows, respectively (left panel). The lesion area is delineated by a dashed line (right panel) Scale bar: 100 µm. (B) Representative micrographs of DIC and ACTA2 staining. Double-head arrows show the thickness of the ACTA2 staining within the area underlaying the lumen defining the fibrous cap area. (C) Quantification of the subluminal ACTA2+ thickness in Myh11-Cre/ERT2 R26R-EYFP Apoe-/- fed a high-fat diet for 18, 21 and 26 weeks. Using this strain of mice, the fibrous cap has an average thickness of 25-30 µm in advance atherosclerotic lesions. Results are expressed as mean ± SEM. (D) Delineation of a fixed 30 µm thick fibrous cap area for single cell counting. Please click here to view a larger version of this figure.

Figure 5: Single cell counting using ImageJ. Screen captures illustrating key steps of single cell counting with ImageJ on images acquired by confocal microscopy. (A) Each individual staining channel and individual z-stack are visible by scrolling c: and z: bars at the bottom of the image. Staining channels are pseudo-colored using the Channel panel (1) Staining channels (YFP, LGALS3, ACTA2, DAPI for nuclear staining and DIC) are merged using the Merge Channel panel (2). (B) Results of channel merging for YFP, LGALS3, ACTA2, DAPI, and DIC. (C) Nucleus counting based on DAPI staining using the Counting icon (1) and Point Tool panel (2). A different counter channel is used for each cell population (3). The number of events counted is indicated below the counter channel (4). White rectangle: region enlarged on the right. (D) Representative image of single cell counting within the fibrous cap area (dashed line) for multiple cell populations including DAPI (yellow dots), YFP+ cells (magenta dots), YFP–LGALS3+ cells (cyan dots), YFP+LGALS3+ cells (orange dots), YFP+ACTA2+ cells (green dots), and YFP–ACTA2+ cells (dark blue dots). White rectangle: region enlarged on the right. Please click here to view a larger version of this figure.
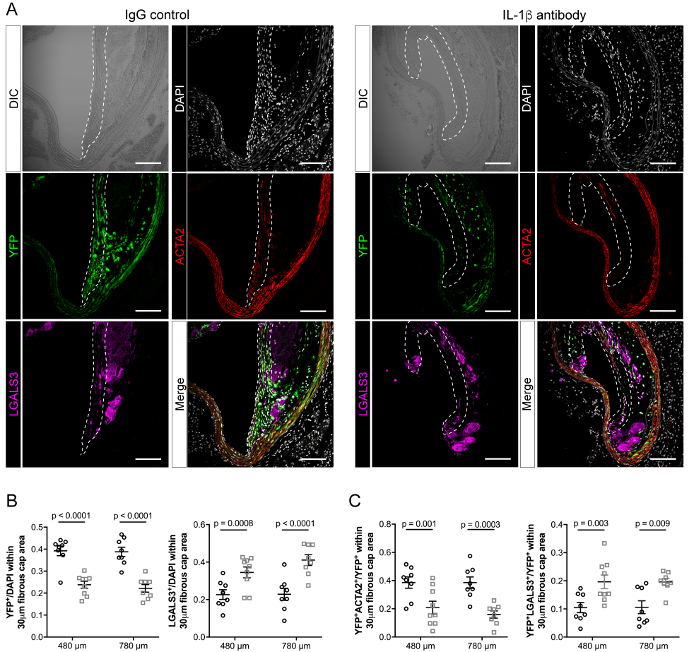
Figure 6: Characterization of the effects of IL-1β inhibition on the cellular composition of the fibrous cap area at two distinct BCA locations of SMC lineage tracing Apoe-/- mice. (A) BCA cross sections at 480 µm and 780 µm from the aortic arch from mice treated with the IL-1β antibody or the IgG control as shown in Figure 1 were stained for YFP, LGALS3, and DAPI (nuclear staining) and the section was imaged by DIC. Immunofluorescent channels were merged (bottom right panels). The dashed lines delineate the fibrous cap regions. Scale bars: 100 µm. (B) Single cell counting reveals that inhibition of IL-1β is associated with a significant decrease in YFP+ cells and an increase in LGALS3+ cells within the fibrous cap area. C) Within the YFP+ cell population, a decrease in YFP+ACTA2+ and an increase in YFP+LGALS3+ populations are observed. Results are expressed as mean ± SEM. Statistical analysis: unpaired multiple t-test. Please click here to view a larger version of this figure.
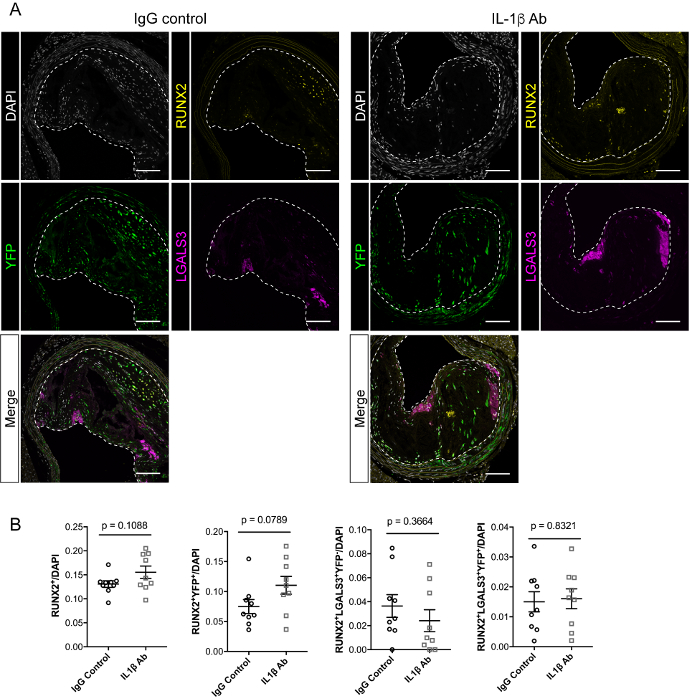
Figure 7: Effect of IL-1β inhibition on the number of RUNX2+ chondrogenic cells with advanced atherosclerotic lesions. A) BCA cross sections are stained for YFP, LGALS3, RUNX2 and DAPI (nuclear staining), and all channels were merged (bottom panels). The dashed lines delineate the lesion area. Scale bars: 100 µm. B) Single cell counting shows that inhibition of IL-1β does not impact the total number of RUNX2+ cells within the lesion nor the proportion of RUNX2+ cells from SMC origin (YFP+RUNX2+; YFP+LGALS3+RUNX2+) and myeloid origin (YFP–LGALS3+RUNX2+). Results are expressed as mean SEM. Statistical analysis: Unpaired multiple t-test. Please click here to view a larger version of this figure.
