Figure 10A shows the occlusal view of a prepared endodontic access cavity in a first maxillary molar after template-aided access cavity preparation of the mesio-buccal canal. Figure 10B shows the insertion of three endodontic handfiles to confirm successful root canal detection after preparation of the palatal and disto-buccal access cavities. After matching the postoperative CBCT data to the preoperative planning data, virtual bur placement generates information about the deviation (Figure 11A). Here, the angular deviation is 0.7°, 0.74 mm 3D deviation at the base of the bur, and 0.87 mm 3D deviation at the tip of the bur. For better visualization, the deviation can be shown in different planes or a 3D-rendered view (Figure 11B).
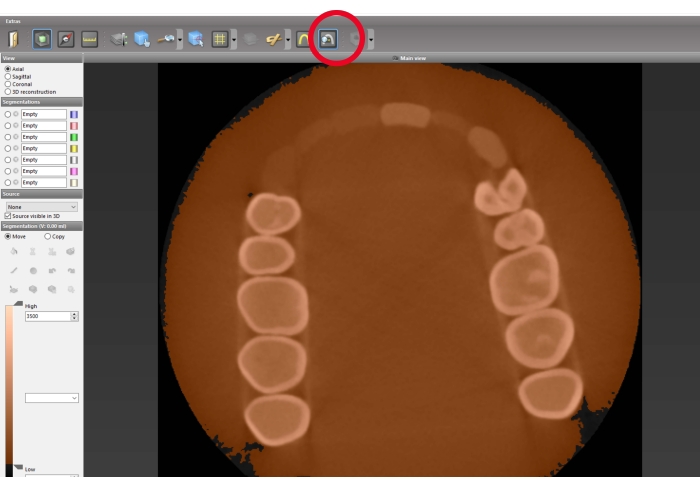
Figure 1: Segmentation preparation. Measurement of the HU density for the tooth enamel and the surrounding material. Calculate the mean value. Red circle: button for the density measuring tool. Left-click to activate, which allows density measurements in the axial view by left-clicking and holding in the desired area. Please click here to view a larger version of this figure.
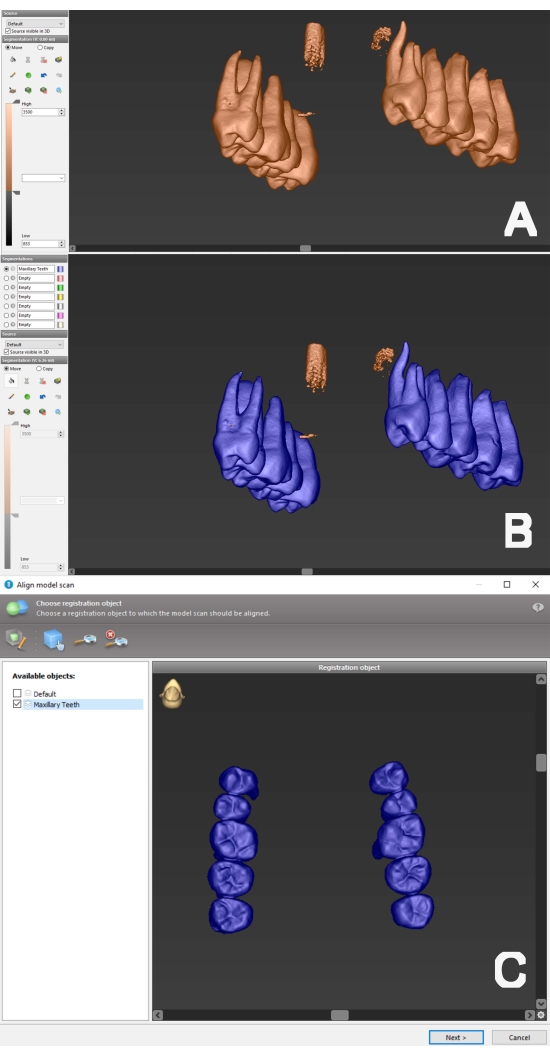
Figure 2: Segmentation process and preparation for alignment with surface data. (A) 3D view of preoperative CBCT data. The lower threshold has been adjusted to the determined mean value. (B) The flood fill tool was utilized to perform a segmentation of the tooth structure (color blue) and was named "Maxillary Teeth". (C) The performed segmentation can be selected (here: "Maxillary Teeth") for the registration step. Please click here to view a larger version of this figure.
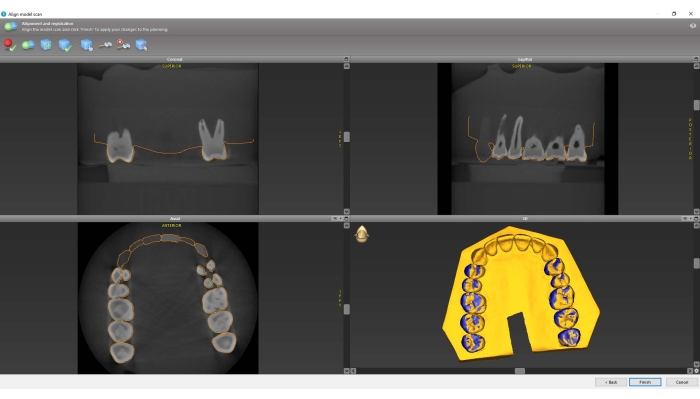
Figure 3: Alignment of CBCT and surface scan datasets. Verify in all planes that matching is accurate and complete the registration step. Note the "camouflage pattern" between segmentation and surface scan data in the 3D reconstruction, which indicates a highly precise matching of the data. Please click here to view a larger version of this figure.
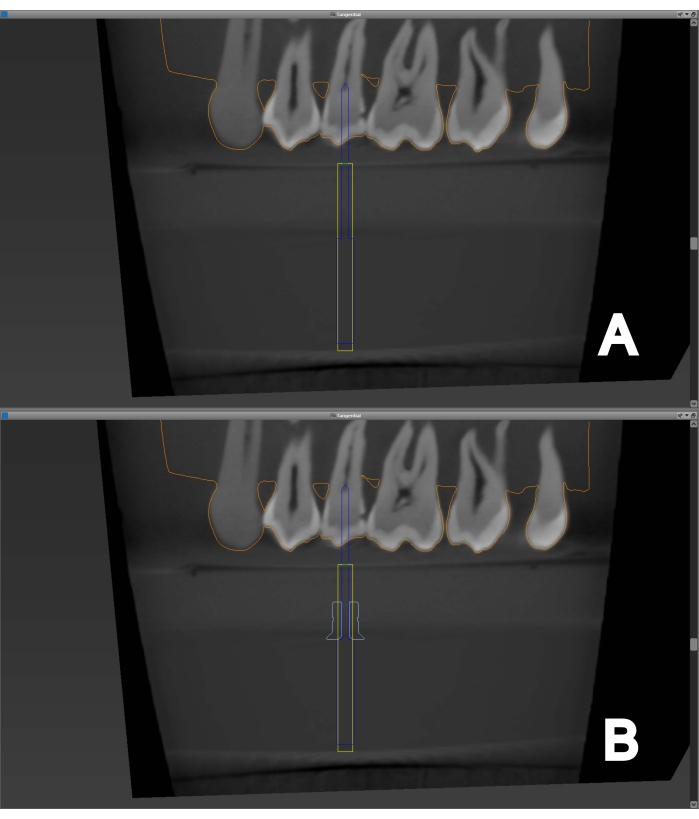
Figure 4: Access cavity planning. (A) An endodontic bur is virtually placed to the root canal orifice of a maxillary second premolar, providing straight-line access. (B) A suitable sleeve can be added to the endodontic bur. There must be enough space between the sleeve and coronal tooth structure to avoid interference when later placing the template on the dental arch. Please click here to view a larger version of this figure.
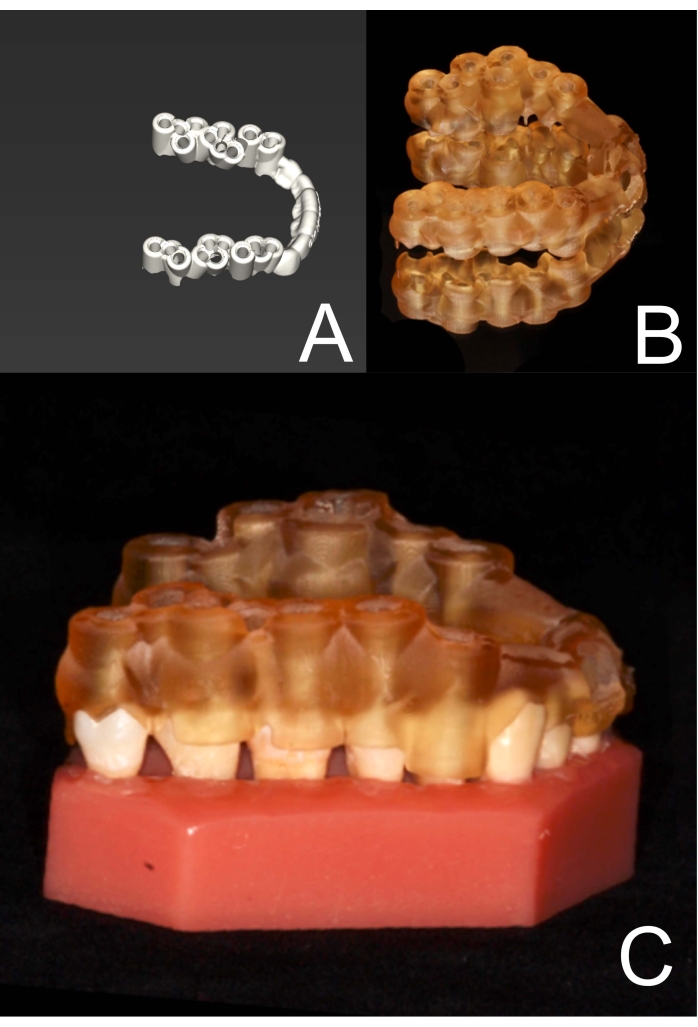
Figure 5: Template for static navigation. (A) The entire template has been designed (here, a maxillary study model with multiple planned access cavities in the posterior tooth area). It is now ready to be exported and 3D printed. (B) The template has been 3D printed. (C) The sufficient fit of the template on the dental arch is checked. Please click here to view a larger version of this figure.
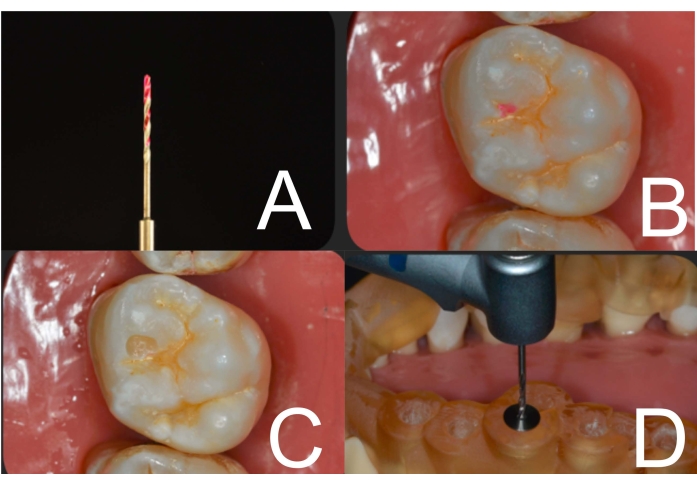
Figure 6: Access cavity preparation. (A) Dye (here: caries detector) at the bur's tip is used to mark enamel at the access cavity site. (B) Enamel has been marked through the template and sleeve. (C) Enamel at the access cavity site has been removed using a diamond bur in a contra-angle handpiece. (D) After sleeve insertion, the template is placed on the dental arch, and the guided endodontic access cavity can be performed with the endodontic bur in a contra-angle handpiece. Please click here to view a larger version of this figure.
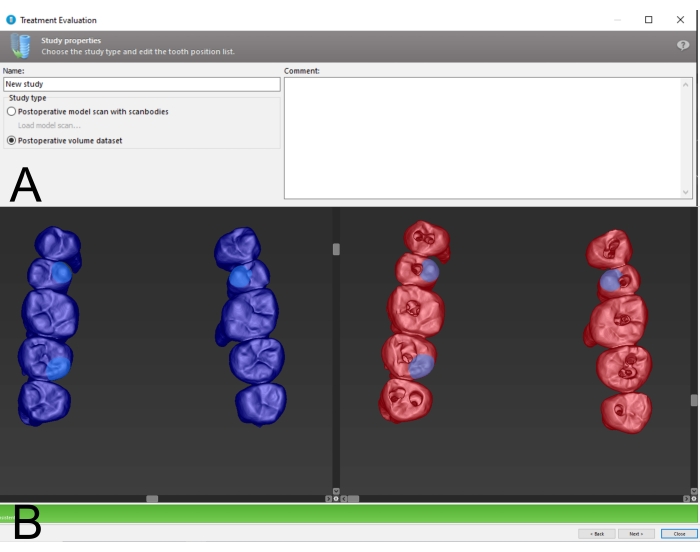
Figure 7: Preparation for treatment evaluation. (A) Choose Postoperative Volume Dataset as a data source for treatment evaluation. (B) Landmark registration between pre- and postoperative CBCT data. Choosing anatomically prominent regions (cusp tips, marginal ridges) as landmarks and their spatial distribution can facilitate semi-automatic registration. Please click here to view a larger version of this figure.
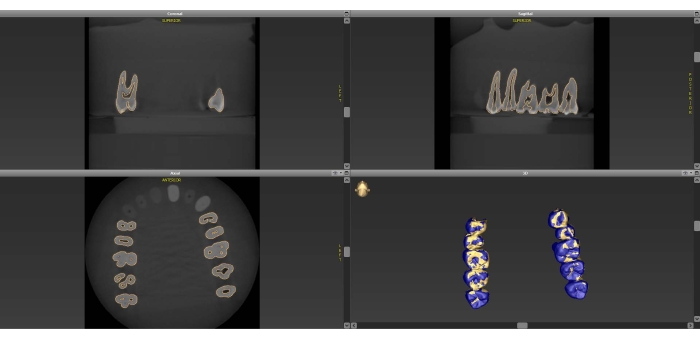
Figure 8: Postoperative CBCT alignment. Matched pre- and postoperative data is shown in all planes and in 3D reconstruction. Note the "camouflage pattern" between the datasets in the 3D Reconstruction, which indicates a highly precise matching of the data. Please click here to view a larger version of this figure.
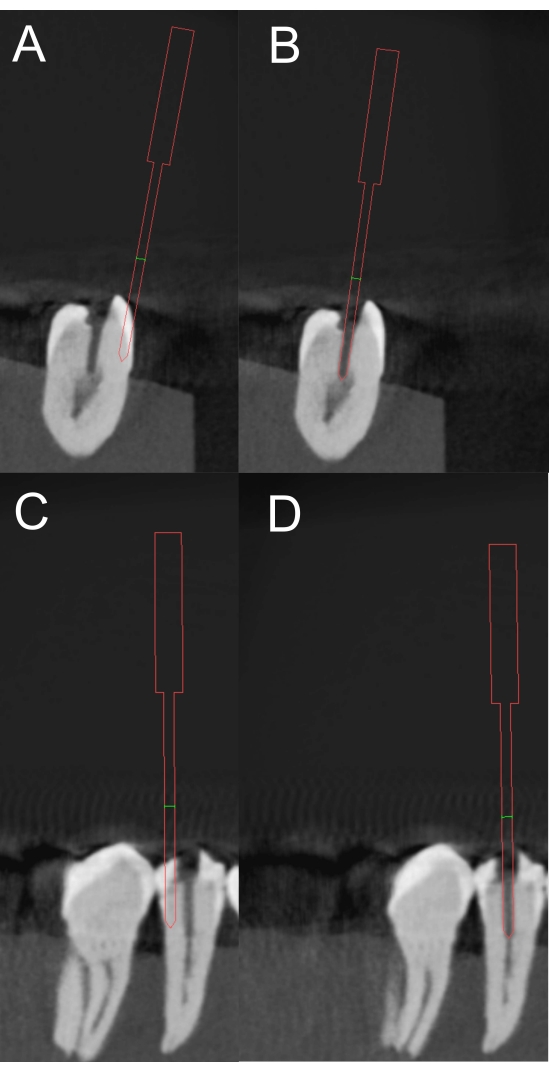
Figure 9: Marking of the access cavity. For treatment evaluation, a virtual bur is placed in the direction of access cavity preparation, which can be withdrawn from the postoperative CBCT data ((A) coronal plane, (C) sagittal plane). Confirm adequate bur positioning in both planes ((B) coronal plane, (D) sagittal plane). Please click here to view a larger version of this figure.
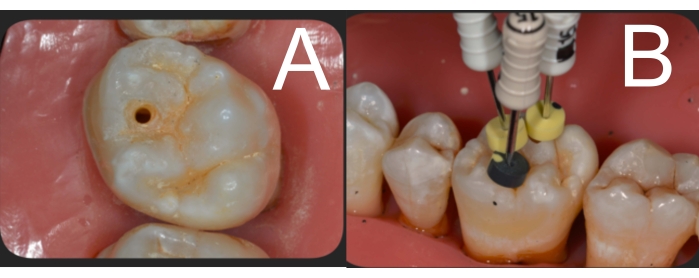
Figure 10: Clinical view after access cavity preparation. (A) Template-aided endodontic access cavity preparation of a maxillary first molar of the mesio-buccal canal. (B) After disto-buccal and palatal root canals are accessed in the same manner, handfiles are inserted to confirm successful root canal detection. Please click here to view a larger version of this figure.

Figure 11: Treatment evaluation. (A) After correct matching of pre- and postoperative CBCT data and correct bur placement, the software calculates the angular and spatial deviation between planned and performed access cavity preparation. The results are presented in a table. (B) Visualization of the deviation is also provided in sagittal or coronal view, or in 3D reconstruction. Please click here to view a larger version of this figure.
Supplementary File 1: A sample stl file of the template. Please click here to download this File.
