Pilot virtual walking group
During COVID-19, an expert working group of seven individuals created and implemented the virtual walking protocol with eight pilot participants. The working group consisted of a PI, a physical therapist, an exercise physiologist, a lab manager, two research study coordinators, and a graduate student. The working group met virtually every week to form a consensus on the methods preceding the pilot of the methods. To pilot the methods, participants from the PD and older adult community were asked to join. Four of the virtual walkers had a diagnosis of PD, and four of the walkers were older adults with no known neurodegenerative disease diagnosis. The virtual pilot walks took place twice per week over a 4 month time frame. Participants were invited to attend any walk during the week. The participant attendance per walk was not recorded at the time, but we had a zero attrition rate during the 4 months of piloting the virtual walk, with no known adverse events. The heart rate and RPE were not measured during this time. The goal of the pilot program was to see if the methodology was feasible and effective in increasing physical activity and social connectivity with the use of technology during the pandemic quarantine. Participant satisfaction surveys were taken at the end of the 4 months (Table 3).
Hybrid virtual/in-person group
As the quarantine measures ended and the COVID-19 vaccine became readily available, in-person walking groups were formed specifically for people at a higher risk for falls and/or who preferred in-person instruction. The pilot participants were invited to continue to join the virtual group weekly. Generally, the enrollment for the virtual and in-person groups was rolling and continuously open, with walking groups being offered five days per week, and each participant walking two times per week for a target goal of 20 walks over a three-month time frame. The in-person and virtual groups included older adults with PD and older adults with pAD. The in-person walking group included people of all mobility levels, from independent ambulators to those requiring assistance due to balance and gait impairments. The virtual group included only participants deemed eligible based on the fall risk screening process.
At the time of authoring this paper, the in-person walking group has six people with PD and four people with pAD, with the expectation for growth as more participants are randomized into the walk intervention of the study. Of the original eight virtual pilot participants, seven are no longer participating due to illness, job obligations, and other personal reasons. For the in-person group, three of the six participants with PD required one-on-one supervision from a trained staff member. Two participants with PD were interested in virtual groups; however, neither of these participants qualified for the virtual walking group due to the high risk for falls. The remaining three of the six participants with PD and all four of the participants with pAD qualified as a low fall risk and, therefore, could walk with less supervision from staff. These seven low-risk participants chose the in-person walking group over the virtual group for unknown reasons. One to two staff members, in addition to the group leader and co-leader, were assigned to the low-fall risk group to monitor for safety and assist the group leader if needed. Typically, the group leader leads virtual participants and the low-fall risk group. All staff assisting with the walk are connected to the group leader and co-leader via a one-tap mobile or conference call line for the duration of the walk. There are 11 total staff members available to support these walks and assigned to walks according to the number of participants who sign up each week. The staff members included research coordinators, physical therapists, personal trainers, exercise physiologists, and graduate students. Additional staff were added over time as the walking group increased in participant size. New staff members were oriented and trained on an informal one-on-one basis by the PI and the staff physical therapist and by the formal balance management training class, as described in the protocol section above. The data presented below were collected from 10 participants with PD or pAD participating in person in walking groups who attended between 4 and 15 classes, at the time of this paper. The demographics and clinical characteristics table (Table 1) shows participants were about 70 years old and relatively highly educated (16-17 years of education). The PD participants had fallen more often in the previous six months compared to the pAD participants. More PD participants used an assistive device and were more afraid of falling than the pAD participants. At the time of this paper, there were no adverse events to report.
Heart rate, RPE, and distance outcomes
As stated in the methods, the heart rate/RPE data from each participant were collected during the in-person walks at five different time points throughout the class: baseline, after the warm up, 15 min, 30 min, and 45 min. At the end of the walk, the distance traveled during the walk was also collected.
The heart rate and RPE of the participants increased over the course of the walk, and people with PD had more variable RPE than those with pAD (Figure 1 and Figure 2). Furthermore, there was a strong positive correlation between RPE and heart rate (Figure 3). A correlation was found between the low RPE scores and HR when the participants were walking at a low to moderate intensity of 50%-75% of their max HR. During these walks, people with PD walked 1,800 m on average, and people with pAD walked 3,000 m on average (Figure 4).
A satisfaction survey was distributed among the pilot virtual participants. These participants were people with PD and with no other known neurological disorder. Five participants responded from a total out of eight consistent walkers who had been with the program over a 4 month time frame. Overall, the program was well-received (Table 3). All members of the group strongly agreed that walking improved their quality of life, motivated them to exercise, contributed to physical well-being, contributed to mental well-being, and that they would recommend the program to a friend or family member. Most participants found the group to be physically challenging. However, a few were neutral or disagreed, possibly due to the nature of the virtual walk. Although participants were verbally cued for intensity ranges based on RPE, ultimately, the pace and route were self-selected by the participant.
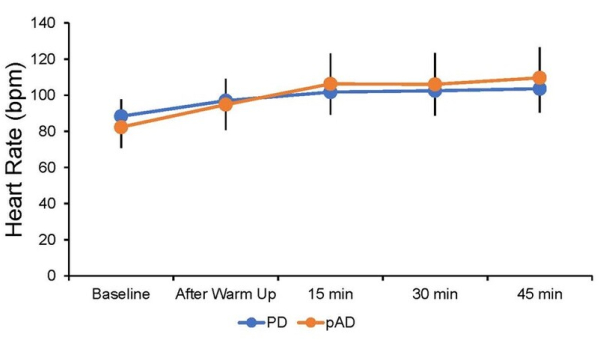
Figure 1: Average heart rates of the PD and pAD participants over the in-person walk. Data collected from multiple in-person sessions for individual participants who attended between 2 and 20 classes. Heart rates were collected at five different time points throughout the class: baseline, after warm up, 15 min, 30 min, and 45 min. Depicted are the average heart rates (± SD) separated by group into individuals with PD (blue; n = 6) and individuals with pAD (orange; n = 4) at each of these time points, with n = 45-57 HR per time point per group. Please click here to view a larger version of this figure.
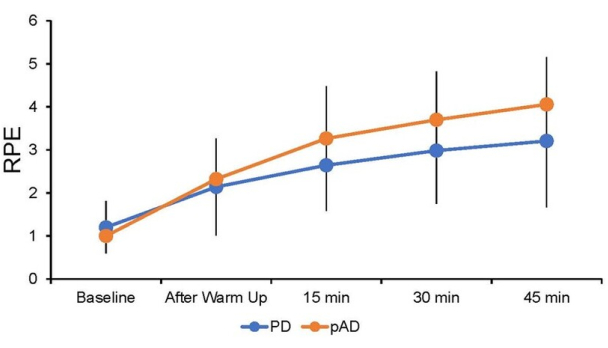
Figure 2: Average rates of perceived exertion (RPE) of the participants during the in-person walk. Data collected from multiple in-person sessions for individual participants who attended between 2 and 20 classes. The RPE was collected at five different time points throughout the class: baseline, after warm up, 15 min, 30 min, and 45 min. Depicted are the average RPEs (± SD) separated by group into individuals with PD (blue; n = 6) and individuals with pAD (orange; n = 4) at each of these time points, with n = 50-59 per time point per group. Please click here to view a larger version of this figure.
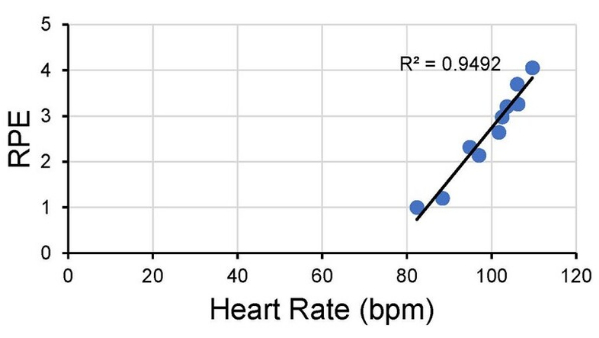
Figure 3: Correlation between the average RPE and heart rate for the different time points over the in-person walk. The average heart rate and average RPE were calculated for the five different time points throughout the in-person walking class and for each group (PD and pAD). These values were then correlated, and an R-squared value was calculated. Please click here to view a larger version of this figure.
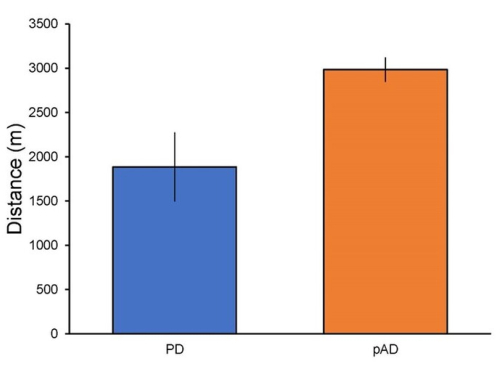
Figure 4: Average distance walked by people with PD and people with pAD in the in-person walk. Depicted is the average distance that the participants walked during the 45 min walking part of the class separated by clinical group (PD: n = 58; pAD: n = 53). This average includes multiple sessions for individual participants who attended between 2 and 20 classes. Please click here to view a larger version of this figure.
Table 1: Demographics table for participants with PD and pAD for the virtual versus in-person walking groups. Please click here to download this Table.
Table 2: Examples of posture and gait cues. Several possible posture and gait cues given at baseline, 15 min, and 30 min of the virtual and in-person walk are presented. Please click here to download this Table.
Table 3: Satisfaction survey. Representative satisfaction survey responses from the original eight virtual walk participants. For example, five out of five of the responding participants strongly agreed that the virtual walk group improved their quality of life. Five out of eight participants responded to the survey. Please click here to download this Table.
