The equations used for mathematically calculating the titer were previously described2,3.
Briefly, for PRRSV, we apply the Karber method:
Titer (TCID50) = 10 T + 1.3 where:

In this formula d = negative log of the last dilution with complete positive virus response: five positive replicates; r = log of dilution range; N = number of replicates by dilution; n = number of wells with positive virus response on the next dilutions.
In the case of IAV, we use the Muench formula:

For details on each mathematical method, refer to Ramakrishnan et al., (2016) and Reed et al., (1938)2,3.
As a visual example, the titer obtained for PRRSV shown in Figure 1 would be calculated as follows:


The number of positive wells obtained when ICC (left half of the plate) and Crystal Violet staining (right part of the plate) were compared was highly similar for both PRRSV (Figure 1) and IAV (Figure 2) and was in both cases able to detect between one and two positive wells more than the CPE observed prior to staining through microscopy, even though these differences were not statistically significant (Table 1). While the output obtained from crystal violet staining is usually a positive-negative well, using ICC there is a gradual decrease on the number of positive cells that get labeled as the virus gets more diluted. Furthermore, ICC requires the use of a microscope for visualization, while crystal violet can be easily performed by eye.
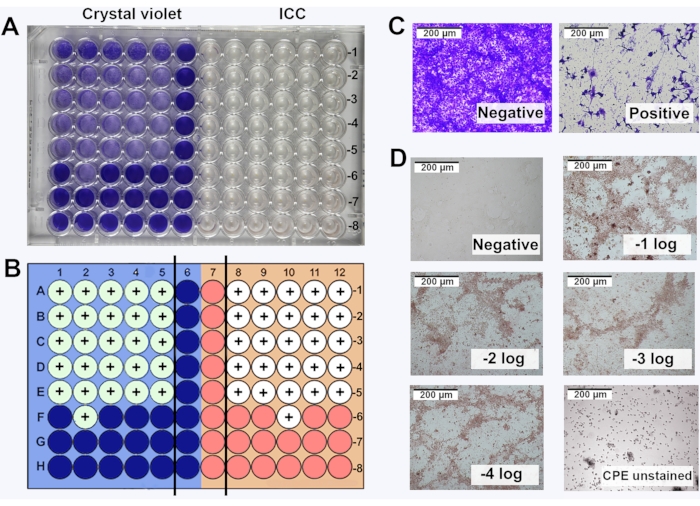
Figure 1: Comparison of crystal violet staining and immunocytochemical labeling (ICC) for PRRSV titration. (A) Visualization of the titration plate by eye, with the left-half corresponding to crystal violet staining and right-half corresponding to ICC; (B) Schematic representation of the plate with positive wells indicated with a '+' sign using crystal violet and ICC; (C) Microscopy image (10x objective) of crystal violet staining; (D) Microscopy image (10x objective) of positive wells detected by ICC. Ten-fold dilutions of the virus from -1 to -8 log. were performed. Images of positive wells from -1 log to -5 log. Uninfected cells were used as negative control (referred as negative). Please click here to view a larger version of this figure.
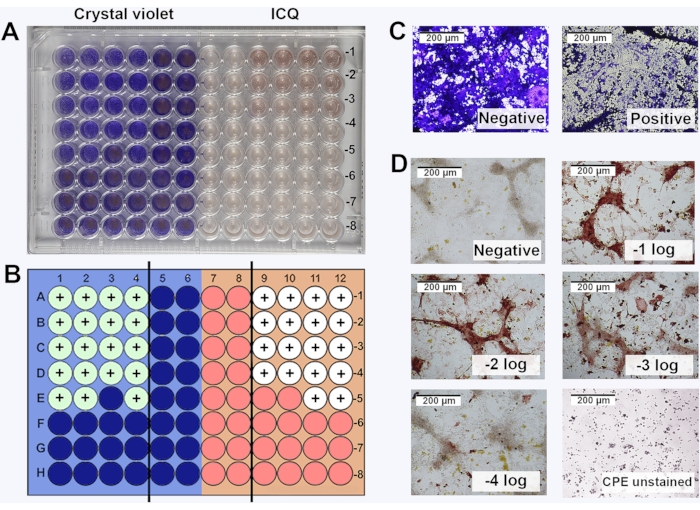
Figure 2: Comparison of crystal violet staining and immunocytochemical labeling (ICC) for IAV titration. (A) Visualization of the titration plate by eye, with the left-half corresponding to crystal violet staining and right-half corresponding to ICC; (B) Schematic representation of the plate with positive wells indicated with a '+' sign using crystal violet and ICC; (C) Microscopy image (10x objective) of crystal violet staining; (D) Microscopy image (10x objective) of positive wells detected by ICC. Ten-fold dilutions of the virus from 10-1 to 10-8. were performed. Images of positive wells from -1 log to -5 log. Uninfected cells were used as negative control (referred as negative). Please click here to view a larger version of this figure.
Table 1: Comparison of the titers obtained for both PRRSV and IAV using the three visualization approaches. Titers expressed as the average ± SEM of the log10 TCID50/mL in n = 5 replicates. No statistically significant differences were found between the groups (p > 0.05). Please click here to download this Table.
