Systemic inflammatory response following PVA sponge implantation
The PVA sponge implantation surgery generated a systemic inflammatory response, as demonstrated by the induction of IL-6 in the plasma 1 day after wounding (Figure 2A). Other proinflammatory cytokines including TNF-α and IL-1β, as well as an array of chemokines including CCL2 and CXCL1 were induced systemically in the first 7 days post-PVA sponge implantation, and have been described elsewhere26,30.
Isolation of cells and fluids from PVA sponge wounds
The primary advantage of the PVA sponge wound model is the ability to recover enough cells for phenotypic and functional analyses of the acute cellular wound healing response. The number of cells that can be recovered from PVA sponge wounds increases over time, from approximately 2 x 106 cells per six sponges on wound day 1 x 106 to 8 x 106 cells on wound day 7 (Figure 2B). The cell number continues to increase beyond day 7. It is not recommended to continue this model beyond ~14 days because the sponges become fully encapsulated by collagen and the system transitions from modeling an acute wound healing response to modeling a foreign body granuloma1,22,23,25,26. Neutrophils, monocytes, and macrophages were the primary cellular infiltrate in PVA sponge wounds. Neutrophils predominated the wound cellular milieu one day after wounding, as assessed by flow cytometric analysis (Figure 2C). Monocytes and monocyte-derived macrophages accumulated within 3 days post-sponge implantation, and the three cell populations increased in number over time (Figure 2C). A representative flow cytometry gating strategy to identify neutrophil, monocyte, and macrophage populations is shown in Figure 2D. After excluding cell doublets using FSC-H and SSC-H parameters (Figure 2D, i and ii), non-viable cells were excluded using an amine-reactive fixable viability dye (shown here) or a nucleic acid dye (e.g., sytox or propidium iodide) (Figure 2D, iii). Residual cellular debris not removed by the prior gating steps was then excluded using FSC-A and SSC-A parameters (Figure 2D, iv). Hematopoietic cells comprised the majority of PVA sponge wound cells and were identified by CD45 expression (Figure 2D, v). Neutrophils were identified as Ly6G+Siglec-F– (Figure 2D, vi). Siglec-F+ cells were primarily eosinophils (Figure 2D, vii). Gating on Ly6G–Siglec-F– cells, monocytes/macrophages were identified as F4/80+ cells (Figure 2D, viii). F4/80+ cells could be further fractionated by Ly6C expression to distinguish Ly6Chi inflammatory monocytes (Figure 2D, ix) and Ly6Clow monocyte-derived macrophages (Figure 2D, x)26.
The ability to measure cytokines and other wound soluble factors is another advantage to the PVA sponge wound model. It is possible to extract up to 100 μL of fluid per sponge. Extracted fluids are suitable for a variety of downstream assays. The detection of cytokines and chemokines in early and late wound fluids by ELISA or bead-based multiplex immunoassays have been reported elsewhere26,30. It is possible to obtain both cells and fluids from the same wound. To do this, it is recommended to isolate three sponges from one side of the dorsal midline for cell isolation and 3 sponges from the opposite side of the dorsal midline for fluid extraction.
Assessment of wound closure using the tail skin excision model
The excisional tail skin model provides an alternative to the dorsal skin punch biopsy method to study slow wound closure in firm skin lacking dense fur. Example images of tail skin wounds at 1, 7, and 15 days post-excision are shown in Figure 3A. Wound closure could be quantified by measuring the area of the wound bed over time. The day 7 and day 15 wound bed areas were approximately 70% and 35%, respectively, of the day 1 wound area (Figure 3B). Full wound closure required approximately 28 days. The tail skin wound could also be observed in cross section by histological analysis. Figure 3C and Figure 3D show representative images of H&E and Masson’s Trichrome-stained tail cross sections, respectively. The lateral margins of the excised skin are indicated by arrowheads on the dorsal surface of the tail.
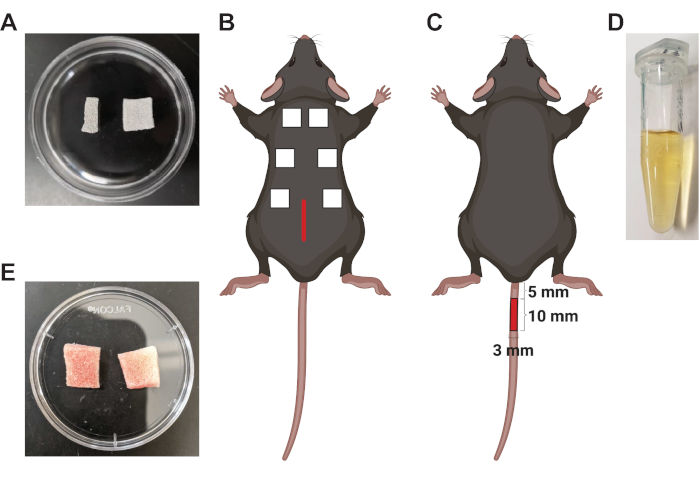
Figure 1: Schematic of murine wound healing models. (A) Side (left) and top (right) view of dehydrated PVA sponges measuring 8 mm x 8 mm x 0.4 mm. (B) Illustration of a mouse demonstrating the placement of the dorsal midline incision (central red line) and six 1 cm x 1 cm x 0.5 cm PVA sponges in subcutaneous pockets. (C) Schematic demonstrating the size and placement of an excisional skin wound (10 mm x 3 mm red rectangle) on the dorsal surface of the tail. (D) Wound fluid isolated from three sponges that were retrieved from the subcutaneous space 7 days after implantation. (E) The appearance of sponges retrieved from the wound 7 days after implantation. Please click here to view a larger version of this figure.
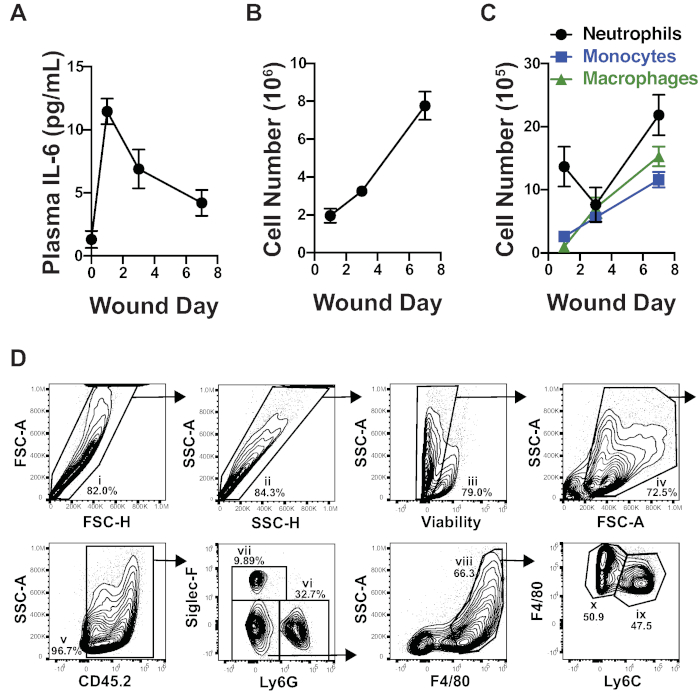
Figure 2: The systemic and cellular response to PVA sponge implantation. (A) A time course of IL-6 levels in the plasma demonstrates that PVA sponge implantation induced a systemic inflammatory response. The concentration of IL-6 was measured using a multiplex bead-based immunoassay. (B) The number of cells isolated from PVA sponges wound increased over time. (C) A time course demonstrates the accumulation of neutrophils, monocytes, and monocyte-derived macrophages in PVA sponge wounds over time. (D) A representative gating strategy of cells isolated from PVA sponge wounds demonstrates how to identify leukocyte subsets by flow cytometric analysis. Gates are defined as follows: (i and ii) doublet exclusion, (iii) dead cell exclusion using an amine-reactive fixable viability dye, (iv) debris exclusion by FSC-A and SSC-A, (v) CD45+ hematopoietic cells, (vi) Ly6G+ neutrophils, (vii) Siglec-F+ eosinophils, (viii) Ly6G–Siglec-F– F4/80+ monocytes/macrophages, (ix) F4/80+Ly6Chi monocytes, and (x) F4/80+Ly6Clow macrophages. Gates were placed according to fluorescence-minus one (FMO) controls. The data shown in A–C are the mean ± SEM, n = 6–10 mice per group in (A), n = 8–9 mice in (B), and n = 6–8 mice in (C). All data are combined from 2–3 independent experiments. Please click here to view a larger version of this figure.
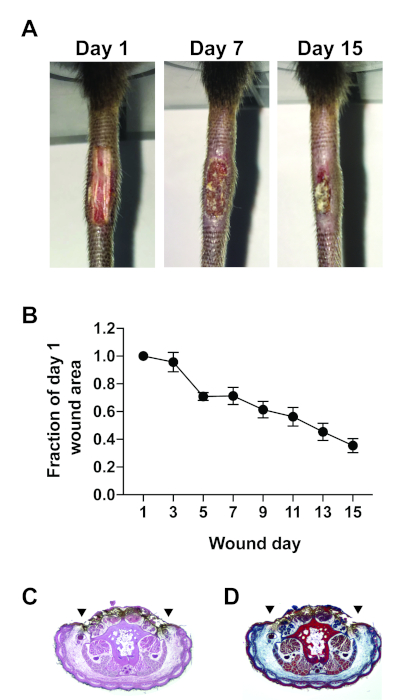
Figure 3: Assessment of excisional tail skin wound healing. (A) Representative photographs of excisional tail skin wounds taken 1, 7, and 15 days post-wounding. (B) The rate of closure of excisional tail skin wounds. Wounds were photographed every other day. Image processing software was used to trace the wound bed margins and calculate the wound area at indicated time points. The wound area is presented as a fraction of the wound area measured on day 1. Representative images of tail cross sections that were paraffin-embedded, sectioned, and stained with (C) H&E or (D) Masson’s Trichrome. The wound was located on the dorsal surface of the tail cross section; lateral wound margins are indicated by arrowheads. The data shown in (B) are the mean ± SEM, n = 8 mice per group. Data are combined from two independent experiments. Please click here to view a larger version of this figure.
