Following the protocol (Figure 1), myocardial ischemia was confirmed immediately by the direct visualization of cyanosis of the epicardium.
Standard ECGs (three limb leads: I, II, and III, and three computed augmented leads: aVL, aVR, and aVF) were recorded continuously pre-ischemia, during ischemia, and at reperfusion (Figure 2). The ECGs demonstrate tachycardia, arrhythmias (i.e., ventricular fibrillation), conduction system defects (i.e., bundle branch block), the development of infarct-related Q waves, and ST segment deviation23.
During regional ischemia, regional hypokinesia was directly observed with the naked eye in the mid cavity of the anterior wall in all the hearts, consistent with the LAD artery's perfusion area that was made ischemic by the restriction of flow with the temporary snaring of the LAD. In both the survival and non-survival cases, 2D ECHO readings were obtained during pre-ischemia, just before inducing regional ischemia, and at different time points during the experiment: 5 min, 10 min, 15 min, 30 min, 60 min, and 120 min. The left ventricular end-diastolic (LVEDD) and left ventricular end-systolic dimensions (LVESD) were measured with a 2D-guided M-mode ECHO at the maximal and minimal LV circumferences, respectively. The regional LV wall contractility in the myocardial ischemic zone was assessed from short-axis views of the LV utilizing M-mode, with the curser line overlying the area at risk. The fractional shortening (FS) was calculated with the following formula: FS = (LVEDD − LVESD)/LVEDD × 10024. The results showed that the fractional shortening decreased during the ischemic time and post-ischemic time compared to the pre-ischemic time (Figure 3)
To quantify the extent of myocardial injury, the infarct size can be measured biochemically with triphenyl tetrazolium chloride (TTC) (Sigma Chemical Co., St. Louis, MO) staining. In this work, the area at risk was delineated by the re-ligation of the involved artery by tying the Prolene stitch left in place. The aorta was cross-clamped, and Monastral Blue pigment (diluted 1:5 in PBS) was delivered through the aorta using a cardioplegia needle. The areas of perfused myocardium were stained blue, and the area at risk remained unstained owing to the ligation of the artery.
The heart was sliced across the long axis of the left ventricle, from apex to base, into 1 cm thick transverse sections, placed between glass plates, and compressed with bulldog clamps. The area at risk for each side of each section was traced on a clear acetate sheet. The heart sections were incubated in a dark container with 1% TTC in phosphate buffer (pH 7.4) at 38 °C for 20 min. The heart sections were then stored in a 10% formaldehyde solution for 24 h before the final measurements to enhance the visualization of the infarct zone. The sections were placed between glass plates and compressed with bulldog clamps. Myocardial necrosis was evidenced by a white area on the myocardial tissue, and the brick-red areas showed the viable tissue. (Figure 4) The infarcted regions (white) within the areas at risk for each side of each section were traced on the clear acetate sheet. Planimetry was used to measure the area at risk and the infarct zone. The volumes of the area at risk and infarcted zone were calculated by multiplying the planimetered areas by the slice thickness. The infarct volume was expressed as a percentage of the total LV volume for each heart25. The ratio of the area at risk to the LV weight was calculated, and the infarct size was expressed as a percentage of the area at risk. Our previous work demonstrated that, after 2 h and 28 days of recovery, the areas at risk (i.e., as a percentage of the LV mass) were approximately 29% and 27%, respectively, for both the mitochondrial and control groups However, after 2 h and 28 days of recovery, the infarct size (i.e., infarct size/area at risk) in the mitochondrial hearts was 9.8% and 7.9%, respectively, compared to 37% and 34% in the control hearts26. Additionally, in our previous experiments, the fractional shortening and LVDP were decreased in the control group to 50%-60% and 70%-80%, respectively, compared to baseline.
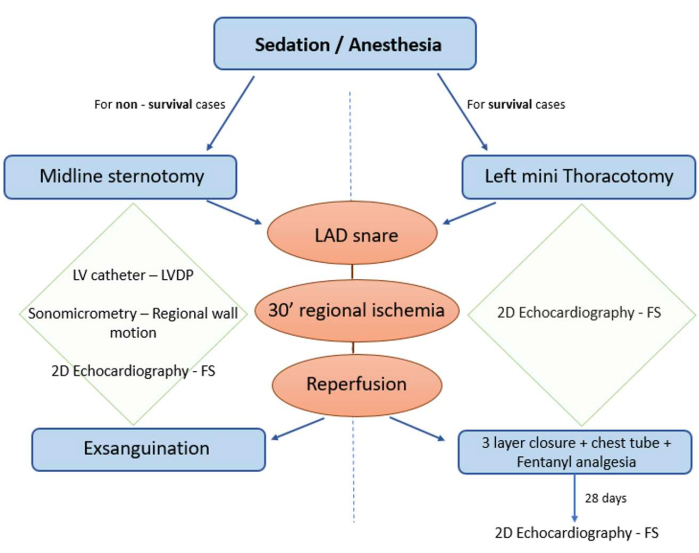
Figure 1: Protocol diagram. The protocol can be adjusted based on the needs of the experiment either for survival or non-survival cases. Non-survival cases can be performed with a more invasive surgical approach using a midline sternotomy, thus allowing for the use of sonomicrometry crystals, epicardial echocardiography (ECHO), and an LV catheter for the measurement of the fractional shortening and LVDP. For survival cases, for which incision healing and pain management must be considered, a left mini-thoracotomy can be performed, and the myocardial function can be assessed at different time points during a longer study period using 2D ECHO. Please click here to view a larger version of this figure.
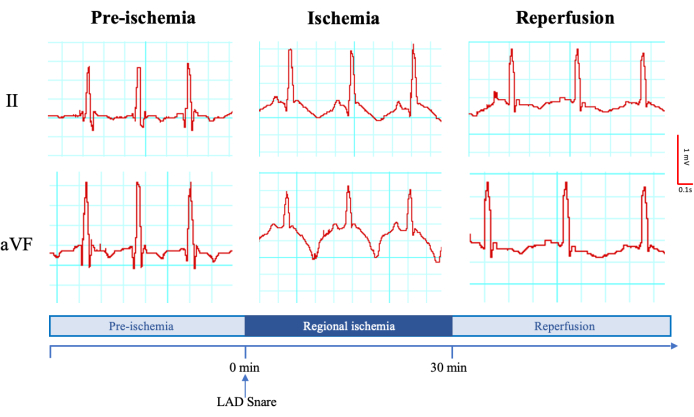
Figure 2: Representative electrocardiogram (limb II and computed augmented lead aVL) before the regional ischemia induction, during the ischemic time, and during the reperfusion. Millivolt and millisecond scales are shown on the left. The time points and the moment of the left anterior descending artery snaring are shown at the bottom. Please click here to view a larger version of this figure.
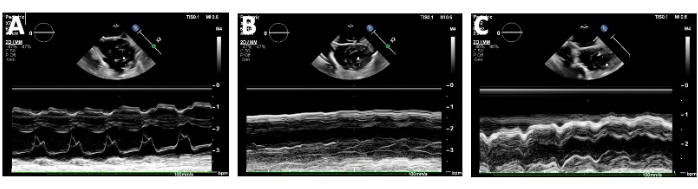
Figure 3: Echocardiographic assessment of the heart by measuring the fractional shortening (FS). The fractional shortening was measured by obtaining the left ventricular end-diastolic distance and the left ventricular end-systolic distance with 2D-guided M-mode at the maximal and minimal LV circumferences, respectively. The fractional shortening was assessed at (A) baseline/pre-ischemia, (B) during the temporary snaring of the left anterior descending (LAD) artery with the cursor line overlying the area at risk, and (C) during reperfusion after releasing the snare on the LAD. Please click here to view a larger version of this figure.

Figure 4: Representative images of the infarct size for a heart stained with 1% triphenyl tetrazolium chloride after 30 min of induced myocardial regional ischemia. The viable tissue is seen as red, while the infarct is seen as white areas. Scale bar = 1 mm. Please click here to view a larger version of this figure.
