There are different approaches to evaluate the outcome of the tMCAo procedure. In vivo neuroimaging methods (MRI) and behavioral testing are utilized here.
Mice develop ischemic lesions in the brain, mainly affecting the territory supplied by the MCA ipsilateral to the occlusion, such as the striatum and dorsolateral cortex. Several methods exist to determine the extent of the lesion, including 2,3,5-triphenyltetrazolium chloride (TTC) tissue staining, histological staining (hematoxylin/eosin, thionine acetate), and in vivo neuroimaging modalities like MRI. MRI has been chosen here due to its non-invasive nature and the ability to use the same tissue for other studies, providing a comprehensive assessment of the lesion in each mouse. Additionally, MRI allows for repeated measurements in the same animals, increasing the reproducibility of results and often reducing the number of animals required for a study.
The same anesthesia protocol with isoflurane (induction 5%, maintenance 1.5%) was used in the MRI sessions. For lesion volume assessment, a fast T2-weighted sequence (T2w turbo RARE fast spin-echo)9 was used to minimize the time the animal is anesthetized, which is important when longitudinal studies with MRI acquisitions at different times are to be performed in the same mice. This procedure allows the evaluation of changes in the lesion over time in the same animals, and it is very useful when applied for neuroprotection studies or to test drug efficacy, among others. Image experiments were conducted on a 7T horizontal animal scanner. The technical specifications of the anatomical sequence (may differ depending on the magnetic field strength): T2_TurboRARE; 22 coronal sections; 0.5 mm thick; echo time (TE) = 33 ms; repetition time (TR) = 2336.39 ms. 2 averages. Flip angle, 90°; field of view (FOV) = 20 mm x 20mm, with a matrix size of 256 x 256. Figure 2A shows a representative example of MR images of lesion evolution in the same mouse, assessed at 40 min, 6 h, 24 h, and 48 h after reperfusion. Progression of the lesion volume takes hours to approximately two days to complete. Quantification of the lesion volume shows this evolution over time (Figure 2B).
A variety of neurological scales have been described to assess the neurological impairment caused by ischemic insult. We suggest using neuroscore tests that have been extensively described in previous manuscripts. For instance, the test reported in detail by Orsini et al. (2012)10 is recommended.
A wide variety of behavioral tests are available, mainly to detect differences in motor and sensory function impairment. For this purpose, the grip strength test and the corner test were used. The grip strength test is used to evaluate motor function. Forelimbs strength is measured with a Grip Strength Meter connected to a digital force transducer (see Table of Materials). Mouse holds on to a horizontal bar with both forepaws while gently pulling it backwards through the tail. The maximum strength of the grip prior to the forepaws release is noted. Five trials per animal are performed, and the main value is calculated after excluding the maximum and the minimum values. The corner test is used to detect unilateral abnormalities of sensory and motor functions. The apparatus consists of a corner with two boards (30 cm × 20 cm × 1 cm) attached with an angle of 30° and a small opening at the end. The mouse is placed halfway facing the corner. When the mouse enters deep into the corner, both sides of the vibrissae are stimulated together. The mouse then turns back to face the open end. A total of 10 trials are performed per animal, and the chosen sides are noted. 50% left and right turns are expected under physiological conditions, whereas a right preference is expected in mice with the right MCAo. A trial is considered valid when a complete turn is achieved or when the mouse turns its head ≥ 90º. Results are shown as the percentage of right (ipsilateral) turns.
The representative results showing the loss of strength exhibited by the mice 24h after tMCAo measured by the grip strength test are presented (Figure 3A), as well as their preference to turn to the side ipsilateral to the lesion when stimulated in the corner test (Figure 3B). Performing behavioral tests on the same day of the surgery may be less precise since some parameters could be altered due to the proximity of the anesthesia and the post-operative period.
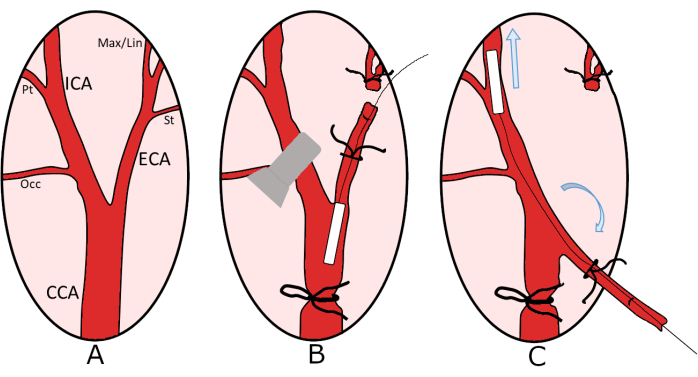
Figure 1: Schematic representation of the vascular tree of the neck (right side). (A) The image shows the main arteries (Common Carotid Artery-CCA, External Carotid Artery-ECA, Internal Carotid Artery-ICA) and the different branches (Pterygopalatine artery Pt; Occipital artery Occ; Superior thyroid artery St; Maxillar and lingual arteries Max/Lin). (B) The first steps of the surgical procedure, with the CCA ligated by suture, the ICA circulation is interrupted by a vascular clamp, and the monofilament is introduced via the ECA. (C) Reorientation of the ECA to push the monofilament to the occlusion zone. Please click here to view a larger version of this figure.
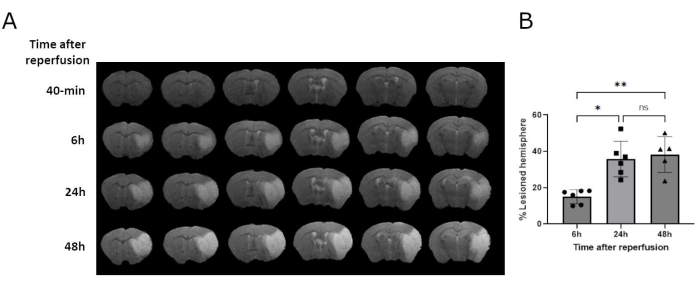
Figure 2: Representative MR images. (A) T2-w images of the same mouse at different time points after reperfusion shows the evolution of the lesion in the acute phase. The area affected by the infarct increases rapidly over the first hours and experiences little variation thereafter. (B) Evolution of lesion volume in the acute phase after MCAo. Each bar represents the mean ± SD of percentage (%) of lesion volume. Lesion volume increases significantly during the first 24 h after reperfusion (*p = 0.0182; **p = 0.0088; 1-way ANOVA/ Kruskal-Wallis test). Please click here to view a larger version of this figure.
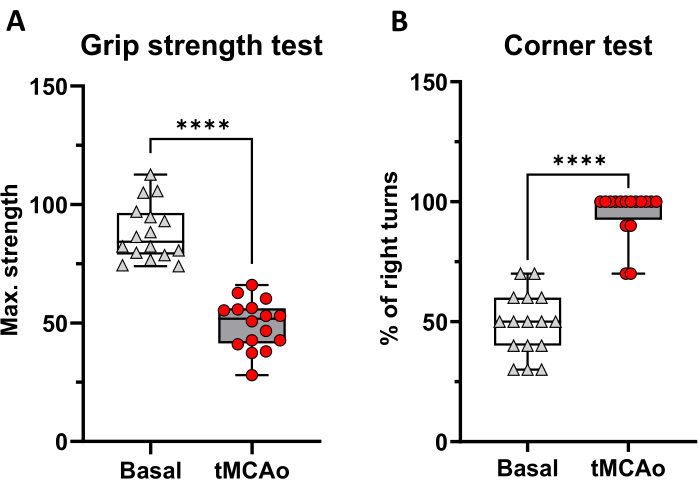
Figure 3: Behavioural tests before (basal) and 24 h after tMCAo (n = 16 mice). (A) Grip strength test shows the maximal (Max.) strength per mouse. (B) Corner test shows the percentage (%) of right turns. Graphs show box and whiskers (minimum to maximum values) per group, and points correspond with individual mice (****p < 0.0001; Wilcoxon matched-pairs signed rank test). Please click here to view a larger version of this figure.
