Pancreas ductaal adenocarcinoom (PDAC) is een van de meest agressieve tumoren en wordt binnenkort de tweede belangrijkste doodsoorzaak 1,2,3. Het staat bekend om zijn immunosuppressieve micro-omgeving en om zijn niet-responsiviteit op immunotherapieprotocollen4. Momenteel is chirurgische resectie nog steeds de enige curatieve optie voor PDAC, maar er is een hoge frequentie van vroege recidieven en postoperatieve complicaties. Het ontbreken van specifieke symptomen tot een vergevorderd stadium maakt een vroege diagnose niet mogelijk, wat bijdraagt aan de deadlines van de ziekte. Bovendien kan de overlap van symptomen tussen PDAC en andere goedaardige pancreaspathologieën het bereiken van een snelle en betrouwbare diagnose met de huidige diagnostische strategieën belemmeren. De identificatie van variabelen geassocieerd met specifieke pancreaspathologieën kan het chirurgische besluitvormingsproces vergemakkelijken en de patiëntprofilering verbeteren.
Veelbelovende resultaten bij het ontdekken van biomarkers zijn bereikt met behulp van gemakkelijk toegankelijke lichaamsvloeistoffen, zoals bloed 5,6,7, urine8, speeksel9 en pancreassap 10,11,12. Veel studies hebben gebruik gemaakt van uitgebreide “omics” -benaderingen, zoals genomische, proteomische en metabolomische technieken, om kandidaat-moleculen of handtekeningen te identificeren die onderscheid kunnen maken tussen PDAC en andere goedaardige pancreasaandoeningen. We hebben onlangs aangetoond dat pancreassap, een relatief onontgonnen lichaamsvloeistof, kan worden gebruikt om metabole handtekeningen van patiënten met verschillende klinische profielen te identificeren12. Pancreassap is een eiwitrijke vloeistof, die het secretoom van pancreaskanaal verzamelt en naar het hoofdkanaal van de pancreas stroomt en vervolgens naar het belangrijkste gemeenschappelijke galkanaal. Vanwege de nabijheid van de alvleesklier kan het sterk worden beïnvloed door micromilieuverstoringen veroorzaakt door de tumormassa (figuur 1), en daarom informatiever dan bloed of urine, of op weefsel gebaseerde profilering. Verschillende studies hebben het potentieel van pancreassap onderzocht om nieuwe biomarkers van ziekten te identificeren met behulp van verschillende benaderingen, waaronder cytologische analyse13, proteomische analyse uitgevoerd door massaspectrometrie14,15, beoordeling van genetische en epigenetische markers zoals K-ras– en p53-mutaties 16,17, veranderingen in DNA-methylatie18 en miRNA’s19 . Technisch gezien kan pancreassap intraoperatief of met minimaal invasieve procedures worden verzameld, zoals endoscopische echografie, retrograde cholangio-pancreatografie of door endoscopische verzameling van duodenale sapsecretie20. Het is nog niet duidelijk in hoeverre de samenstelling van pancreassap wordt beïnvloed door de gebruikte verzameltechniek. We beschrijven hier de intraoperatieve verzamelprocedure en tonen aan dat pancreassap een kostbare bron kan zijn voor PDAC-biomarkers.
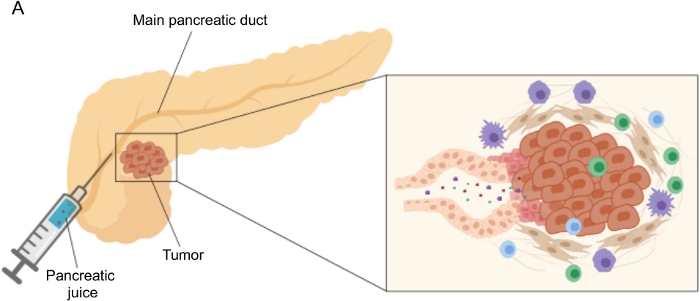
Figuur 1: Schematische weergave van de verzameling van pancreassap. (A) Schematische weergave van de afscheiding van pancreassap in de pancreaskanalen en de verzameling ervan tijdens de operatie. De inzet toont een close-up van de micro-omgeving van de tumor: pancreassap verzamelt moleculen die vrijkomen door tumor- en stromale cellen in de pancreaskanalen. Klik hier om een grotere versie van deze figuur te bekijken.
Het verzamelen van pancreassap in genetische en orthotopische muismodellen van PDAC zou worden gewaardeerd in het perspectief om deze biofluïde te exploiteren in preklinische mechanistische studies; deze procedure kan echter technisch zeer uitdagend zijn en is niet haalbaar voor eenvoudigere modellen zoals subcutane tumoren. Om deze reden identificeerden we tumor interstitiële vloeistof (TIF) als een alternatieve bron voor pancreassap, vanwege het vergelijkbare kenmerk van het fungeren als een indicator van omliggende verstoringen. Interstitiële vloeistof (IF) is de extracellulaire vloeistof, gevonden buiten bloed- en lymfevaten, die weefselcellen baadt21. ALS de samenstelling wordt beïnvloed door zowel de bloedcirculatie naar het orgaan als de lokale secretie; in feite produceren en scheiden omliggende cellen actief eiwitten af in de IF21. Het interstitium weerspiegelt micromilieuveranderingen van omliggende weefsels en kan daarom een waardevolle bron zijn voor biomarkerontdekking in verschillende pathologische contexten, zoals tumoren. De hoge concentratie van lokaal uitgescheiden eiwitten in TIF kan worden gebruikt om kandidaat-moleculen te identificeren die moeten worden getest als prognostische of diagnostische biomarkers in plasma 22,23,24. Verschillende studies hebben aangetoond dat TIF een geschikt monster is voor proteomische benaderingen met hoge doorvoer, zoals massaspectrometrietechnieken23,24,25, evenals multiplex ELISA-benaderingen26 en microRNA-profilering27.
Er zijn verschillende benaderingen voorgesteld voor de isolatie van IF in tumoren, die in grote lijnen kunnen worden gecategoriseerd als in vivo (capillaire ultrafiltratie 28,29,30,31 en microdialyse 32,33,34,35) en ex vivo methoden (weefselcentrifugatie 22,36,37,38 en weefselelution 39,40,41,42). Deze technieken zijn uitgebreid besproken43,44. Bij de keuze van de geschikte methode moet rekening worden gehouden met zaken als de downstreamanalyses en -toepassingen en het teruggewonnen volume. We hebben deze aanpak onlangs gebruikt als een proof of principle om de verschillende metabole activiteit van tumoren van twee muizen pancreas adenocarcinoom cellijnen12 aan te tonen. Op basis van literatuur24,38 hebben we ervoor gekozen om de lage snelheid centrifugatiemethode te gebruiken om celbreuk en verdunning door intracellulaire inhoud te voorkomen. Zowel de hoeveelheid glucose als lactaat in TIF weerspiegelden de verschillende glycolytische kenmerken van de twee verschillende cellijnen. Hier beschrijven we in detail het protocol voor de twee meest gebruikte methoden voor de isolatie van TIF: weefselcentrifugatie en weefselelutie (figuur 2).
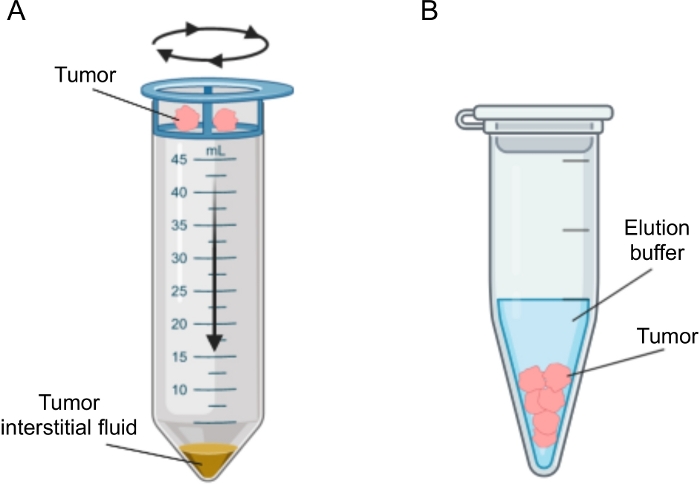
Figuur 2: Schematische weergave van tumor interstitiële vloeistofisolatiemethoden. Schematische illustratie van de in detail beschreven technieken in het protocol, namelijk weefselcentrifugatie (A) en weefselelutie (B). Klik hier om een grotere versie van deze figuur te bekijken.
