Establishment of surgical procedure
A total of 17 animals were utilized for this experiment: 14 mice were employed for optimizing the organ procurement process, including cannulation of the portal vein (PV) and bile duct (BD), while 3 mice were used to validate the procedure (Table 1). Histological results (Figure 3) were compared to facilitate the identification of the optimal perfusion condition.
Selection of perfusate
A previously utilized hepatocyte culture medium was selected for this study10,11. William's E medium was initially designed by Williams and Gunn as a serum-reduced medium for prolonged in vitro cultivation of mature rat liver epithelial cells12. Nonetheless, it has also found utility in supporting the growth and maintenance of rodent hepatocytes13. Fetal bovine serum (FBS) is a widely employed cell culture supplement due to its rich composition of essential nutrients and growth factors that facilitate cell growth, proliferation, and viability14. Complete William's E medium was used as the perfusate (Table 2), which is supplemented with 20% fetal bovine serum, 1 % penicillin/streptomycin, 5,000 U/L heparin, 50 U/L insulin, and 0.010 g/L hydrocortisone.
Selection of cannula
The cannulation procedure involved first cannulating the bile duct (BD) for bile fluid collection, followed by the cannulation of the portal vein (PV). For BD cannulation, a UT-03 polypropylene tube with an outer diameter of 0.3 mm and an inner diameter of 0.18 mm was initially used. However, due to concerns regarding potential BD damage and the higher risk of unintended catheter displacement associated with the trimmed and rigid UT-03 tip, a preference was given to the 1 Fr polyurethane tubes. The polyurethane tubes, with their softer material and reduced slipperiness, were considered more suitable for BD cannulation.
Initially, a 26 G polypropylene intravenous needle cannula was used for cannulating the portal vein (PV). However, the removal of the needle and subsequent attachment of the cannula to the perfusion tube resulted in the formation of bubbles, which had the potential to obstruct the intrahepatic sinusoids. To overcome this issue, an indwelling cannula was constructed using a 30 G needle inserted into the distal 1 cm of a 2 Fr polyurethane cannula. This self-made "needle-guided cannula" was then inserted into the distal PV above the confluence. As the catheter was positioned within the PV, the needle was slowly withdrawn while simultaneously advancing the tube. The end of the self-made cannula was connected to the perfusion tube inside the chamber. Using a soft material in this cannulation technique provided an advantage by reducing the risk of injury to the vessel's back wall.
Validation studies
Inlet and outlet perfusate samples were subjected to the determination of pH and potassium levels. The obtained results (Figure 4) were then compared to the findings reported in recent publications15,16,17. Three mouse livers were perfused with oxygenated and supplemented with William's E medium for 12 h. Throughout this period, a stable perfusion pressure of 7 – 10 mmHg was continuously recorded. The mean pH was relatively stable throughout the 12 h perfusion and ranged between 7.3 and 7.7. Mean potassium levels were also stable throughout the perfusion period and ranged between 5.9 and 6.8 mmol/L (Figure 4). The PV flow rate was maintained within a range of 0.8 – 1.2 mL/min/g depending on the usage and positioning of pump tubes during the experimental procedures. All results observed in mouse liver perfusion demonstrated similarities with previously reported observations in rat liver perfusion (Table 3).
Tissue samples were collected from three livers (N = 3) and were subjected to 12 h perfusion using the optimized protocol for HE-staining, followed by whole slide scanning. Each liver lobe was scored using a modified Suzuki score (Table 4). The classic Suzuki score18 was augmented by incorporating three additional parameters: pyknosis of nuclei, detachment of vessels, and presence of erythrocytes in sinusoids and large vessels. Each parameter was graded as absent (0), mild (1), moderate (2), and severe (3). A final score of 0 – 7 was considered to reflect good preservation, 8 – 14 was taken as moderate preservation, and 14 – 21 indicated bad preservation.
Preservation of the mouse livers was assessed based on the modified Suzuki score. Two medical experts conducted an independent assessment of the morphology of the seven lobes of the three livers (Figure 5, Figure 6, Figure 7). The average of the seven lobe scores for each liver lobe was calculated; lower scores indicate a better-preserved liver. The evaluations rendered by the experts exhibited a high degree of concordance. Notably, while slight discrepancies in the scores assigned by the two experts were observed in the assessment of pyknosis of nuclei, these variations did not impact the overall scoring outcomes significantly.
At best, the liver parenchyma was relatively intact with a well-preserved typical lobular structure, hardly distinguishable from a normal liver. Hepatocytes appeared viable with clearly visible cell membranes and round nuclei. However, some nuclei underwent pyknosis, and some hepatic sinusoids were slightly dilated, resulting in a score of 4. (Figure 3, Figure 6)
At worst, the lobular structure was distorted, with vessels detached from the parenchyma and confluent parenchymal necrosis. On the cellular level, cellular vacuolization, and nuclei pyknosis became obvious, especially in the pericentral region. Furthermore, mild to moderate vacuolization was observed. Up to 30 % of the hepatocytes were undergoing necrosis resulting in a maximal score of 14. (Figure 3, Figure 7)
Table 1: Step-by-step establishment of a mouse liver perfusion model. Various complications were observed during the establishment process due to differences in cannula size, material, and positioning. Please click here to download this Table.
Table 2: Comparison of in vitro organ preservation methods15,17,19,20,21,22. The optimization of perfusate selection, oxygen carrier selection, and nutritional component comparison is crucial under various storage conditions. Please click here to download this Table.
Table 3: Hemodynamics and blood gas analysis in normal rats and rat NEVLP11,15,16,17,18,20,21,23,24,25,26,27,28,29,30,31. The provided information selectively describes the hemodynamic features of rat liver and key parameters of normothermic perfusion in vitro. Specifically, the rat liver perfusion can be considered optimal when the PV pressure typically ranges from 4 to 10 mmHg, and the partial pressure of oxygen in the perfusate entering the PV ranges from 80 to 550 mmHg, meeting the necessary criteria for successful in vitro rat liver perfusion. Please click here to download this Table.
Table 4: Modified Suzuki score. The modified Suzuki score used in this study expands upon the classic Suzuki score by incorporating three additional parameters: pyknosis of nuclei, detachment of vessels, and the presence of erythrocytes in sinusoids and large vessels. Each parameter was assigned a grade on a scale of 0 (absent), 1 (mild), 2 (moderate), or 3 (severe). The total score, ranging from 0 to 8, indicates good preservation; 9 to 16 suggests moderate preservation, and 17 to 24 indicates poor preservation. Please click here to download this Table.
Table 5: Selection of perfusate medium, perfusate volume, and perfusion pressure based on a literature workup of NEVLP in rats (2010-2022)3,8,10,14,17,19,27,30,31,32,33,34,35,36,37,38,
39,40,41,42,43,44,45. Normothermic machine perfusion in rat liver can exhibit variability across studies in terms of the specific type and volume of perfusate utilized, as well as the duration of perfusion. Different studies may employ varying approaches, such as dialysis or high-volume perfusion, for extended periods. However, despite these differences, parameters such as portal pressure, portal vein flow rate, and partial pressure of oxygen in the perfusate generally demonstrate minimal variation across the various methods employed. Please click here to download this Table.
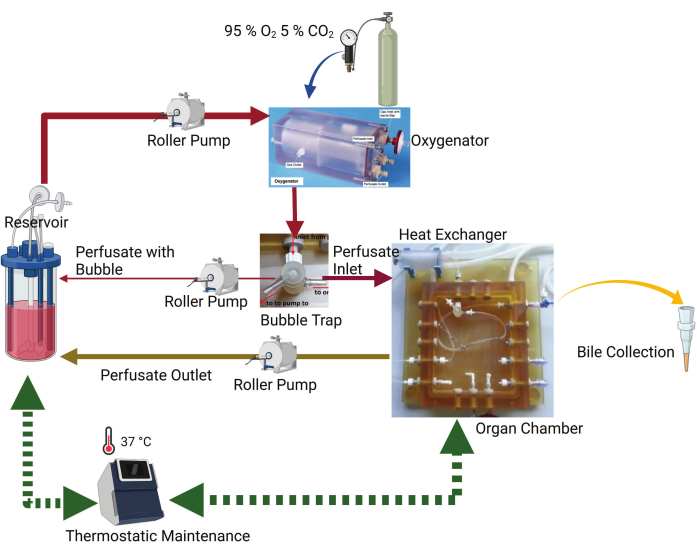
Figure 1: Schematic diagram of the perfusion system. The key components are the organ chamber, thermostatic machine, roller pump, oxygenator, and reservoir. The perfusate is pumped from the reservoir by a peristaltic pump into an oxygenator. There is an uninterrupted gas flow of 95% O2 and 5% CO2 in the oxygenator. The perfusate passes through the bubble trap, where any air bubbles present in the perfusate are captured and pumped back to the reservoir. The remaining perfusate flows to the organ chamber, where the tube is connected to the portal vein. The perfusate outflow from the organ chamber is directed back to the reservoir by the peristaltic pump. A bile drainage tube is connected to the organ chamber to collect bile. Please click here to view a larger version of this figure.
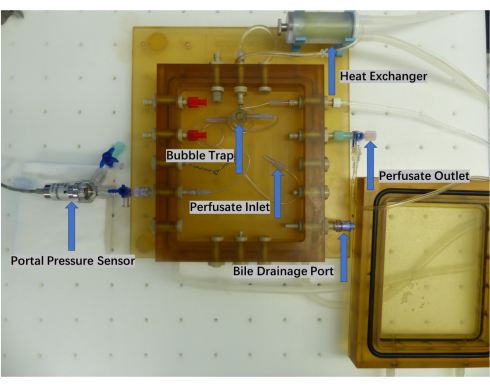
Figure 2: Close-up of the perfusion chamber. The organ perfusion chamber comprises a perfusate inlet and outlet, a bubble trap, a heat exchanger, and a bile collection port. Real-time monitoring of the perfusate pump pressure is accomplished using a pressure sensor. Please click here to view a larger version of this figure.
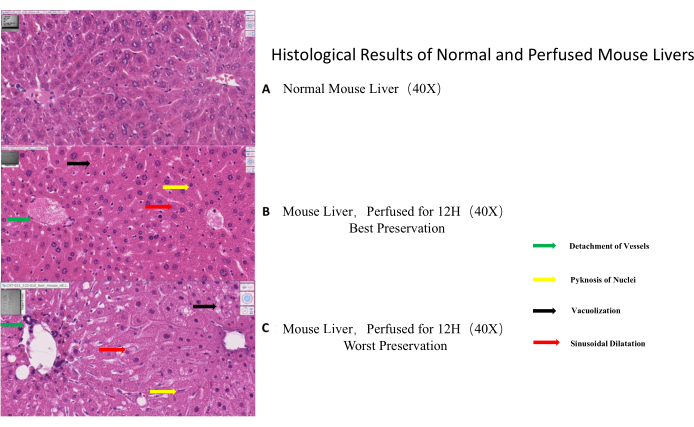
Figure 3: Histological results of normal and perfused mouse livers. (A) Normal mouse liver morphology (control). (B) Example of best-preserved morphology as visualized by HE-staining after 12 h of perfusion. (C). Example of worst-preserved morphology as visualized by HE-staining after 12 h of perfusion. The black arrow indicates vacuolization, the red arrow points to sinusoidal dilatation, the yellow arrow shows pyknosis of nuclei and the green arrow specifies vascular detachment. Please click here to view a larger version of this figure.
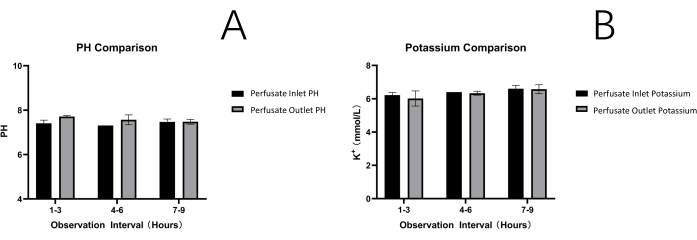
Figure 4: Perfusate analysis. Ph (A) and potassium levels (B). Both parameters are stable throughout the observation times of 12 h, indicating constant perfusion conditions Please click here to view a larger version of this figure.
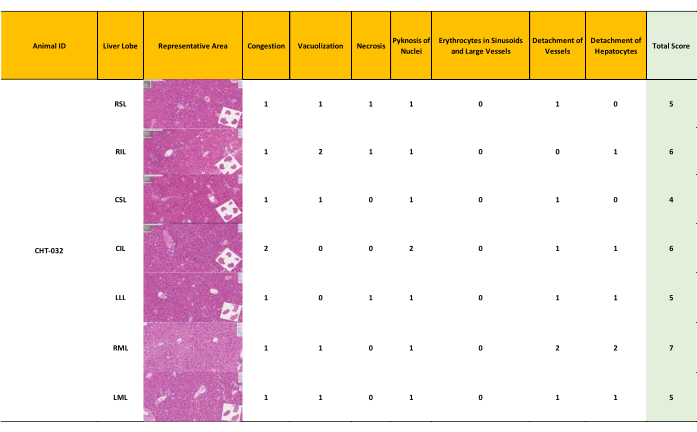
Figure 5: Minor liver damage resulting in a modified Suzuki score 4-7. After 12 hours of NEVLP, a semiquantitative assessment of liver morphology was conducted. Samples from each liver lobe were assessed and graded separately, resulting in a range and a mean score for each liver, with the highest possible score being 4. Well-preserved liver morphology with a score ranging from 4-7 depending on the liver lobe (mean = 5) (Score 0-7: well-preserved liver morphology, score 8-14 moderately preserved morphology, score 15-21: ill-preserved liver morphology) Please click here to view a larger version of this figure.
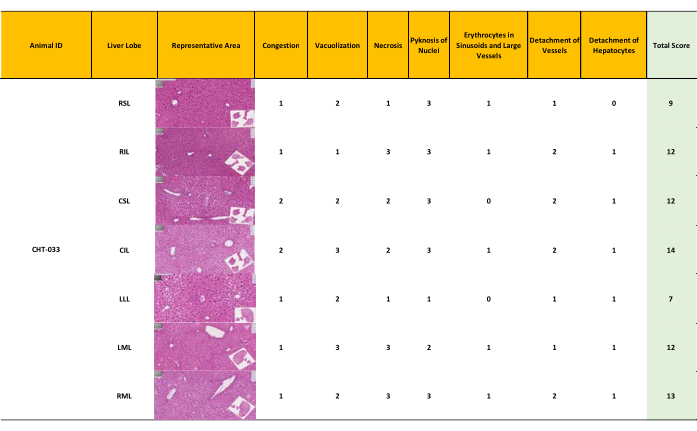
Figure 6: Moderate liver damage resulting in a modified Suzuki score 7-14. Semiquantitative assessment of liver morphology after 12 hours of normothermic oxygenated machine perfusion according to the modified Suzuki score. Moderately preserved morphology with a score ranging from 7 to 14 (mean = 11). (Score 0-7: well-preserved liver morphology, score 8-14 moderately preserved morphology, score 15-21: ill-preserved liver morphology) Please click here to view a larger version of this figure.
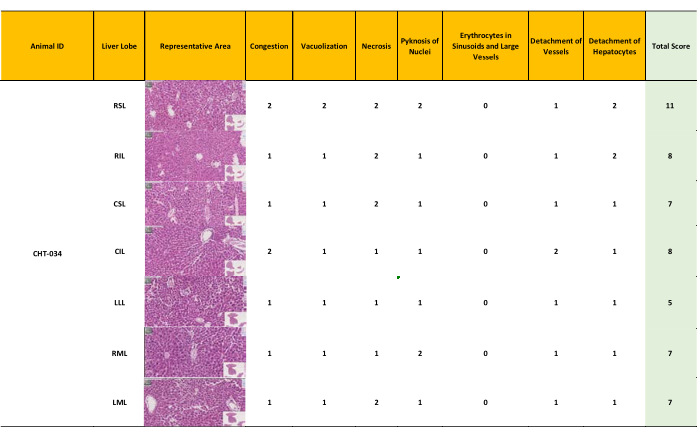
Figure 7: Minor – moderate liver damage resulting in a modified Suzuki score 5-11. The inhomogeneous perfusion resulted in minor to moderate preserved morphology in different liver lobes, with scores ranging from 5 to 11 (mean = 8). (Score 0-7: well-preserved liver morphology, score 8-14 moderately preserved morphology, score 15-21: ill-preserved liver morphology) Please click here to view a larger version of this figure.
