Recent results indicate that in one consecutive series of 78 patients who underwent SEEG insertion via robotic assistance had successful localization of the EZ in 76.2% of patients.1 That same study showed of the patients who went on to have surgical resection of EZ had grade 1 Engel seizure freedom in 67.8% of patients (Figure 4). Morbidity rate is 2.5%. Permanent morbidity was noticed is 1 patient (1.2%). Per electrode, it was shown to have a wound infection and intracranial hematoma rate of 0.08%, each.
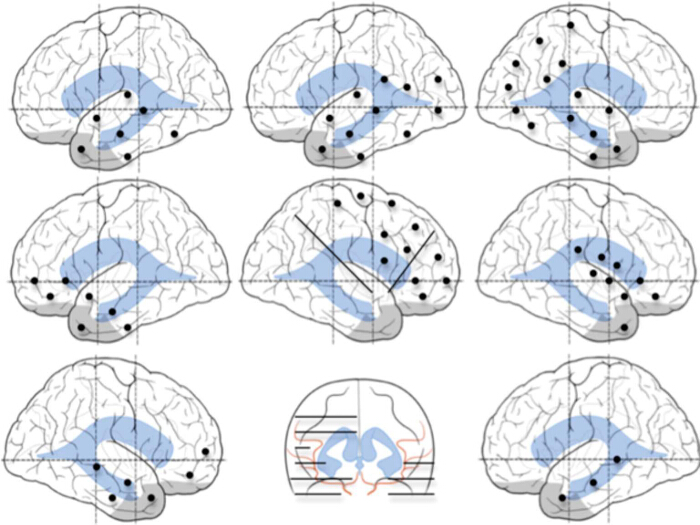
Figure 1. Examples of Patterns of SEEG Implantations. All Insertions are Individual Customized Based on the Patient's Proposed Hypothesis. In these examples we show (from top to bottom, left to right) temporal, temporal-occipital, temporal-parietal-occipital, fronto-temporal, fronto-parietal-insular, perisylvian, and frontal and bitemporal insertion plans. Black dots represent entry points of SEEG electrodes, implanted in orthogonal fashion. Black lines represent electrode trajectories. Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography. Copyright 2011 – 2013. All rights reserved. Please click here to view a larger version of this figure.
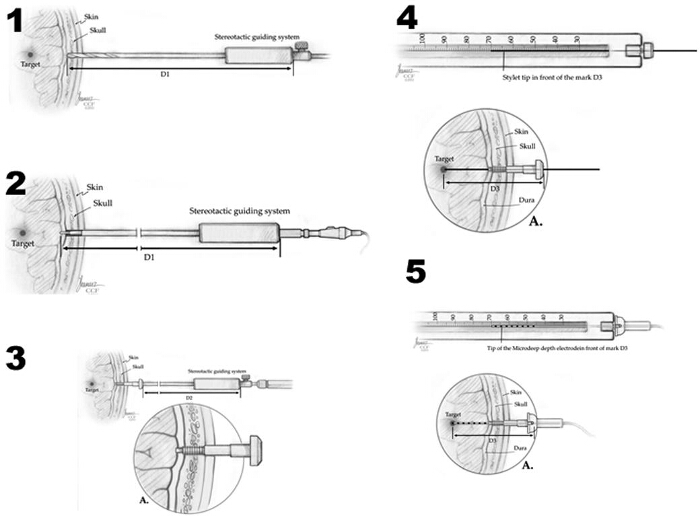
Figure 2. Method of Depth Electrode Implantation. 1) The skull is drilled with a 2.5-mm drill bit, guided by the stereotactic system. 2) The monopolar coagulator probe is inserted and the dura is opened. 3) The implantation bolt is screwed into the skull, also guided by the stereotactic system. 4) The final depth distance for the electrode (D3) is calculated and measured: [(Target-Dura Distance + D1) – D2 = D3]. Initially, the trajectory is created by a stylette probe, guided by the implanted bolt. 5) Final position of the depth electrode, and its fixation into the bolt, preventing displacements and CSF leaks. Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography. Copyright 2011-2013. All rights reserved. Please click here to view a larger version of this figure.
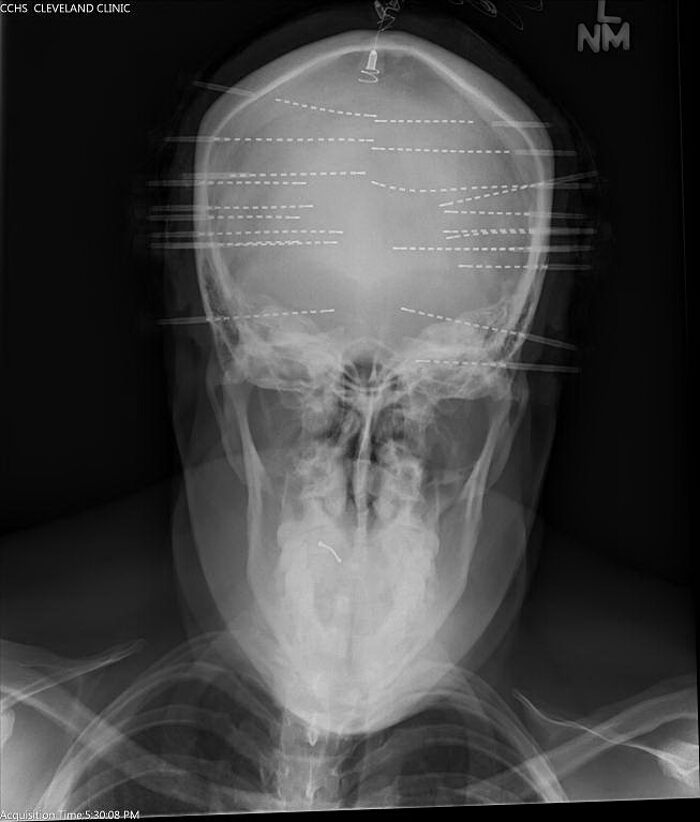
Figure 3. Intraoperative Operative AP Skull X-ray. Obtained to confirm placement of electrodes corresponds with preplanned trajectories. Please click here to view a larger version of this figure.
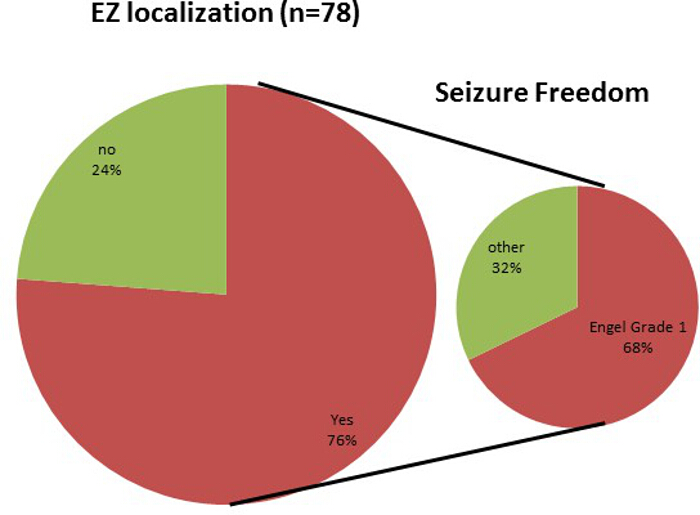
Figure 4. Outcomes of Patients Undergoing SEEG Monitoring. Seventy six patients were able to have their EZ localized; furthermore of those patients undergoing resection after SEEG 67% experienced Engel Grade 1 seizure freedom. Please click here to view a larger version of this figure.
