The LoCoSP device is a useful tool for safely dissecting the structures of the upper mediastinum. Direct visualization of the cervical and upper thoracic esophagus allows for safe dissection with less risk of tracheal injury and hemorrhage from tearing of the larger vessels, in addition to improving the lymphadenectomy of the left recurrent laryngeal and paratracheal nodes.
From 2018 to 2020, 12 patients with distal esophageal carcinoma (2 squamous cell carcinoma and 10 adenocarcinoma) were submitted to laparoscopic transhiatal esophagectomy with transcervical access to cervical esophagus dissection and lymphadenectomy. The median age was 62 (60 ± 85) years old, only one patient was female. There was no chordal palsy, bleeding, tracheal damage related to the transcervical access. One anastomotic fistula occurred with no clinical complications, spontaneous drainage through the cervical incision. The median operation time was 360 min (300 ± 420 min), and the operation time of the transcervical dissection of the cervical esophagus was 60 min (40 ± 110 min). The median hospital stay was 10 days (9 ± 12 days). All cases were performed with the LoCoSP device (Table 1).

Figure 1: Low-cost single-port device Please click here to view a larger version of this figure.
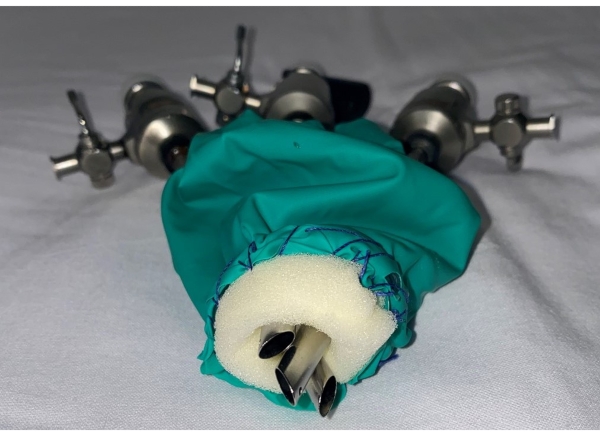
Figure 2: Low-cost single-port device (note the triangulation of the three trocars) Please click here to view a larger version of this figure.
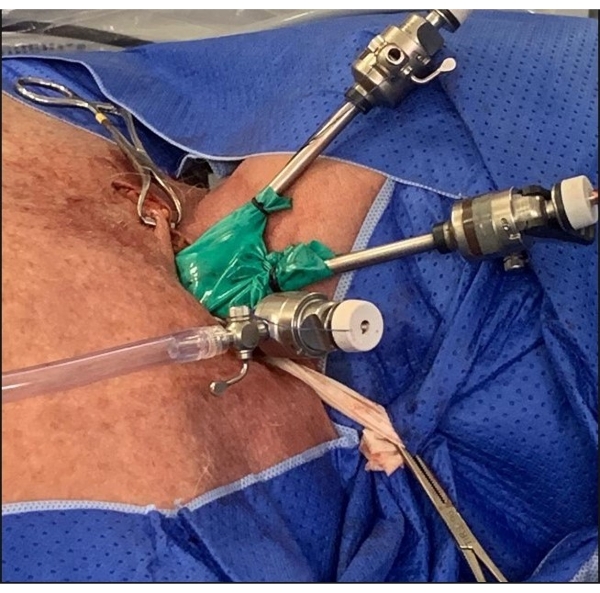
Figure 3: Low-cost single-port device into the cervical wound Please click here to view a larger version of this figure.
| Total Patients | 12 |
| Median Age (years) | 62 |
| Number Anastomotic fistula | 1 |
| Median operation time (minutes) | 360 |
| Median operation time transcervical dissection (minutes) | 60 |
| Median Hospital stay (days) | 10 |
Table 1: Surgery results using low cost single-port device
