The use of this protocol with the recommended stimulation settings, under inhalation anesthesia with isoflurane 2.0% oxygen 0.8 L/min, should produce results as shown in Figure 11 and Figure12, where there is multiple back to back stimulations between 75-80 mm Hg. Figure 13 shows the same stable response over a 20-min stimulation with the response stable at 73-77 mm Hg. Test the line for ICP measurement by flushing the tube and tapping on the crus (Figure 9). The rapid response back to baseline is the hallmark of a well-placed line. If the integrity of the tunica albuginea is damaged, the test would result in lower peak pressure and slow response back to baseline after flushing and tapping, and a diminished response when stimulating (Figure 14). There would also be leakage of the heparinized NaCl when flushing and bleeding during stimulations.
The types and levels of anesthesia as well as the use of oxygen had a major impact on ICP. Figure 15 demonstrates the effect of the different levels of isoflurane on ICP, with both a decreased response and a less stable plateau. With isoflurane at 2%, there was a stable response in the ICP measurement with multiple stimulations on 78 mm Hg. Increasing the concentration of isoflurane to 3.5%, however, resulted in a rapid 50% decrease to 34 mm Hg in multiple, subsequent stimulations. The same effect was observed when switching the isoflurane from 2.0% to 3.0%, where a 19% decrease in response was observed, and from 2.5% to 5%, where an even more rapid decrease in response of 70% was seen. Blood pressure remained stable throughout all stimulations. In rats anesthetized using the isoflurane/oxygen anesthesia during surgery and initial stimulations, who then received 25% of the recommended dose of fentanyl/midazolam (while the isoflurane was discontinued), there was a similarly stable response but it increased by 25% during the fentanyl/midazolam anesthesia compared to isoflurane (Figure 16).
Administration of oxygen through a nose cone increased the oxygen saturation in the blood from 61-75% to 99-100% in about 20 s. When the oxygenation was stopped, the same decrease was seen over approximately 1 min. Blood pressure was stable throughout the stimulations, but oxygen administration through a nose cone (0.8 L/min) had a large effect on the maximum ICP measurement, reducing it by 35-45% in back-to-back stimulations (Figure 17).
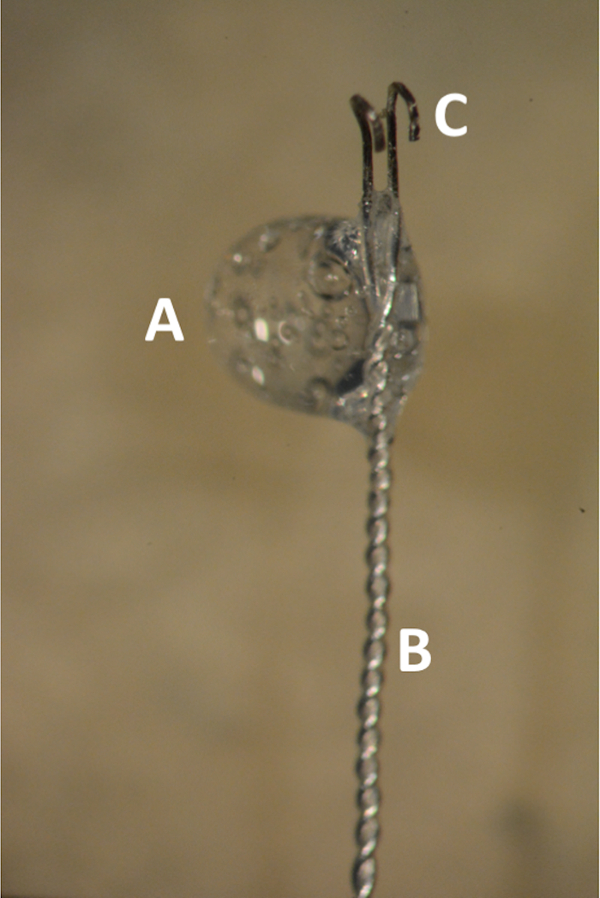
Figure 1. The bipolar Teflon coated silver electrode. (A) Glue bubble in the transition zone between the coated and uncoated electrode. (B) Distal 2 cm of the electrode tightly braded. (C) Parallel uncoated hooks 1 mm apart. Please click here to view a larger version of this figure.
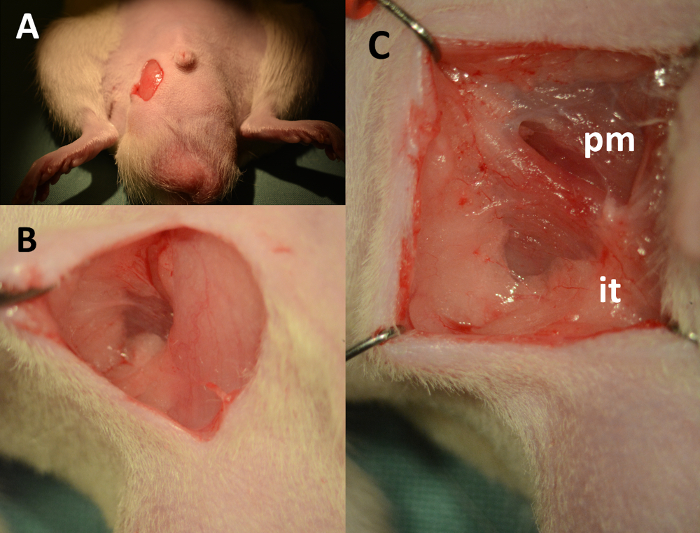
Figure 2. Dissection of the cavernous body – landmarks. (A) 1 cm vertical skin incision, downward starting 2 mm lateral from the base of the penis. (B) Fascia lateral to the scrotum separated using cotton-tipped swabs. (C) View of the operating field after placement of retractors (pm: pyramidalis muscle, it: insertion point of crus to the ischial tuberosity). Please click here to view a larger version of this figure.
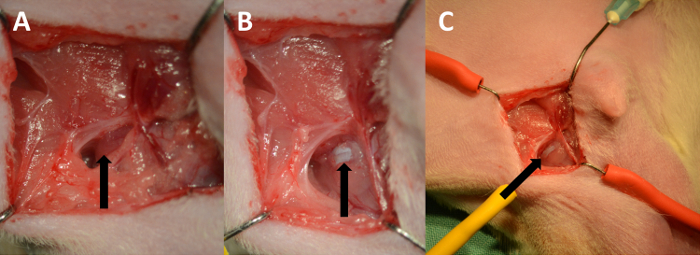
Figure 3. Exposing the tunica albuginea. (A) The ischiocavernosus muscle (arrow). (B) Tunica albuginea (arrow). (C) Low power magnification showing the course of the cavernous body. Please click here to view a larger version of this figure.
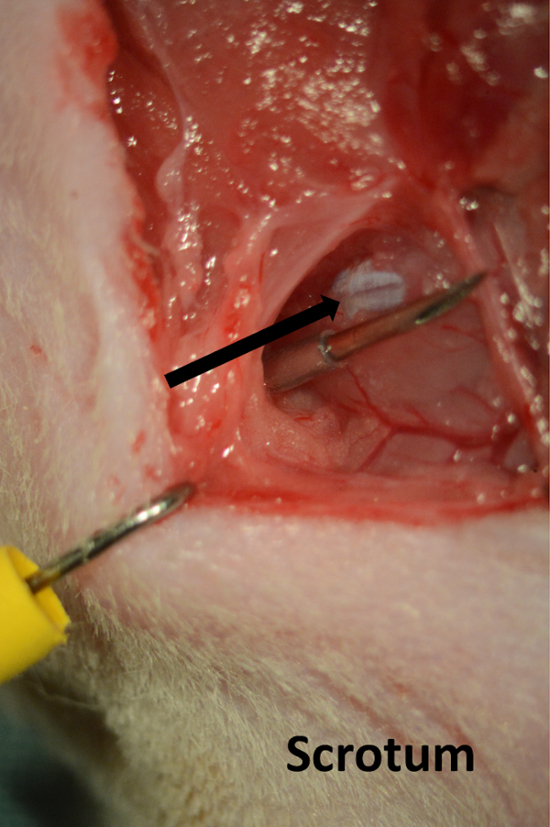
Figure 4. Line for cavernous pressure recording. Needle introduced through the skin on the perineum running parallel with cavernous body (arrow). Please click here to view a larger version of this figure.
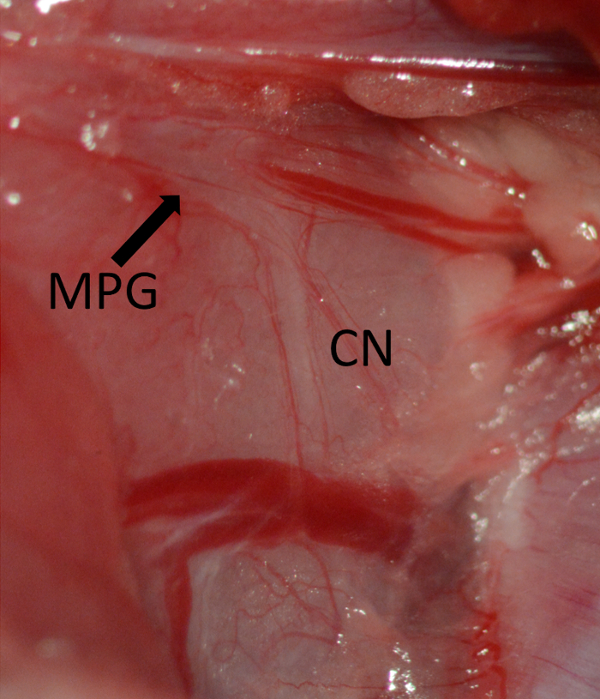
Figure 5. Exposure of the MPG marked by arrow and CN running vertical on the dorsolateral aspect of the prostate. Major pelvic ganglion (MPG) marked by arrow, cavernous nerve (CN). Please click here to view a larger version of this figure.
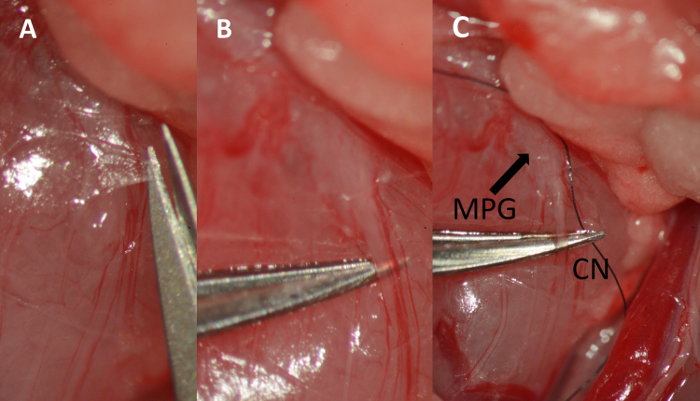
Figure 6. Dissection of the cavernous nerve. (A) Cutting the fascia overlying the cavernous nerve with micro scissors. (B) Separating the nerve from the underlying tissue using micro forceps. (C) Placing a 9-0 ligature underneath the nerve. Major pelvic ganglion (MPG) marked by arrow, cavernous nerve (CN). Please click here to view a larger version of this figure.
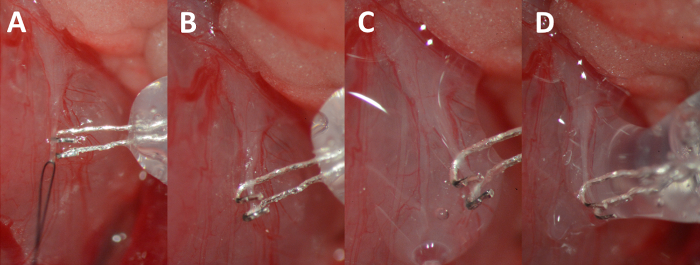
Figure 7. Hooking of the nerve. (A) Elevating the nerve by gently pulling on the suture. (B) Nerve resting in the hooks of the electrode. (C) Nerve and electrode complex isolated with the biocompatible silicon glue. (D) Additional glue bubble added to completely isolate the nerve-electrode complex. Please click here to view a larger version of this figure.
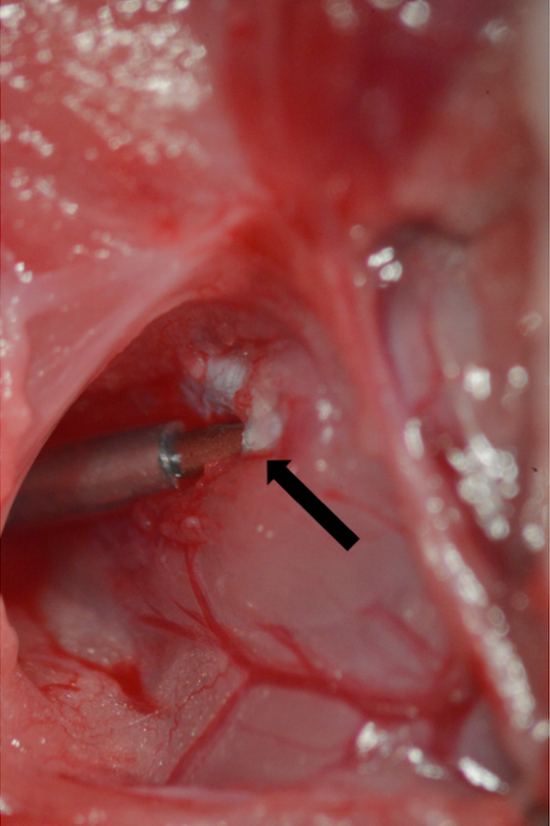
Figure 8. Cannulation of the tunica albuginea. A 23 G needle connected to PE-50 tubing inserted into the tunica albuginea. Point of insertion marked by arrow. Please click here to view a larger version of this figure.
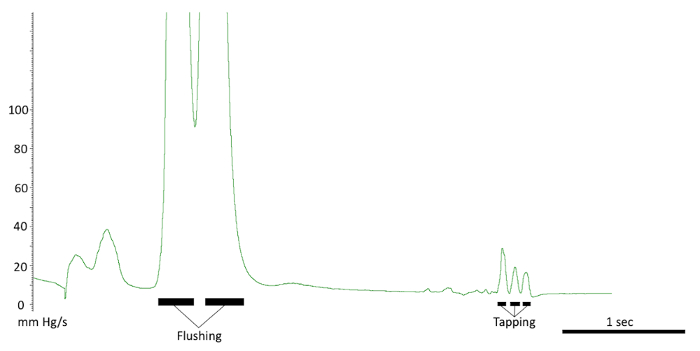
Figure 9. Testing the intracavernous line. The responses seen with a correct line placement. Note the flushing of the line and response to tapping on the crus. Also, note the quick pressure drop back to baseline. Please click here to view a larger version of this figure.
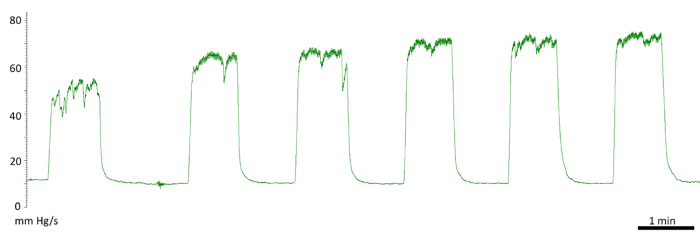
Figure 10. Initial responses to cavernous nerve stimulation. Diminished first response. First stimulation of 50 mm Hg and a fluctuating plateau. Second and third stimulation of 66 mm Hg. The following measurements were recorded at the normal level at 73 mm Hg. Please click here to view a larger version of this figure.
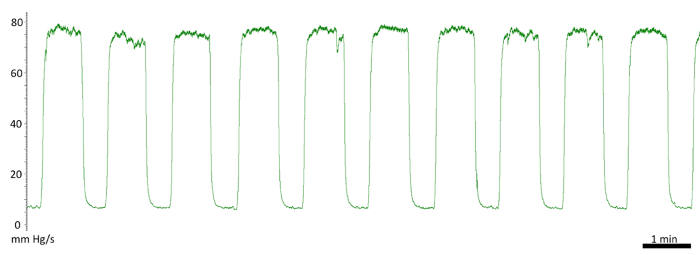
Figure 11. Repeated cavernous nerve stimulation and intracavernous pressure recording. Showing the stability of the results using this protocol. Ten back-to-back stimulations between 75-78 mm Hg. Please click here to view a larger version of this figure.
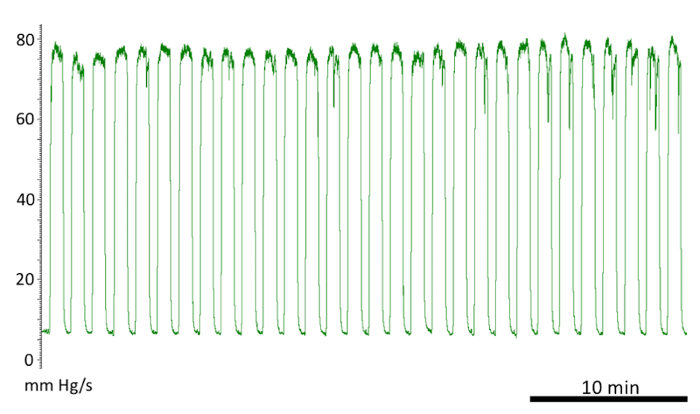
Figure 12. Cavernous nerve stimulation and pressure recording. Approximately 30 back-to-back stimulations with < 6 mm Hg variability in the pressure. Please click here to view a larger version of this figure.
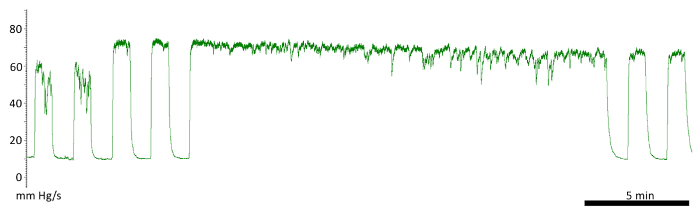
Figure 13. Continuous stimulation lasting 20 min. Increased fluctuation at the end, but the subsequent stimulations, after a 1 min rest, produced a stable response. Please click here to view a larger version of this figure.
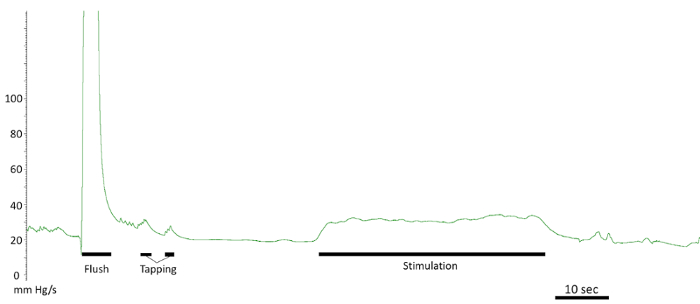
Figure 14. Leaking tunica albuginea. Prolonged response back to baseline after flushing and tapping. Decreased response after stimulation. Please click here to view a larger version of this figure.
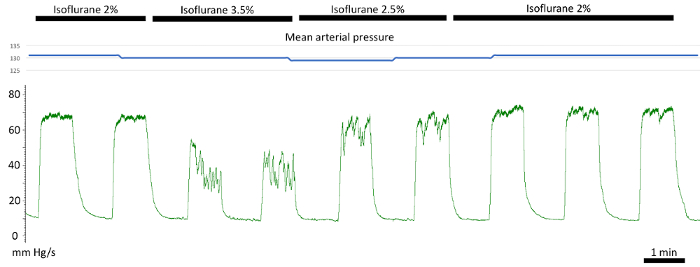
Figure 15. The effect of anesthesia dose on intracavernous pressure. Decreased and more fluctuating response on increasing isoflurane compared to the stable response on 2% in the first two, and the last three stimulations. The blue trace on top showing constant mean arterial pressure. Please click here to view a larger version of this figure.
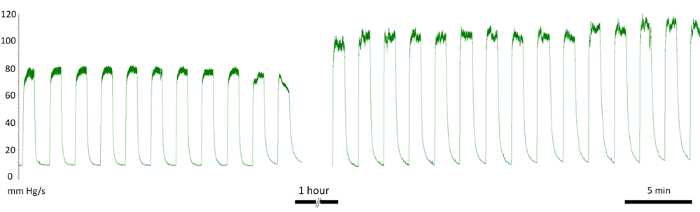
Figure 16. The effect of anesthesia type on intracavernous pressure. The initial stimulations performed under isoflurane anesthesia show a pressure increase of 80 mm Hg, once fentanyl/midazolam was administered there was an increase in response to 110 mm Hg. Please click here to view a larger version of this figure.
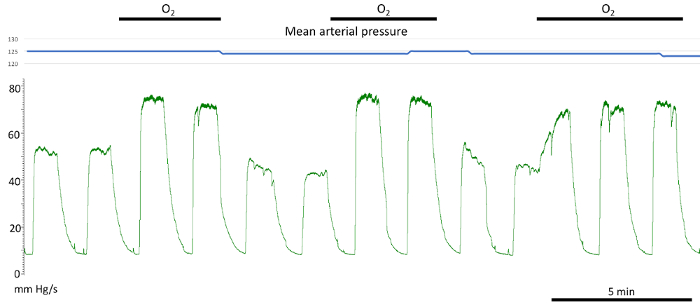
Figure 17. The effect of oxygen administration through the nose cone. Discontinuing oxygen administration through the nose cone resulted in a significant reduction in cavernous pressure increase with cavernous nerve stimulation. No effect on the mean arterial pressure was noted (blue trace above). Please click here to view a larger version of this figure.
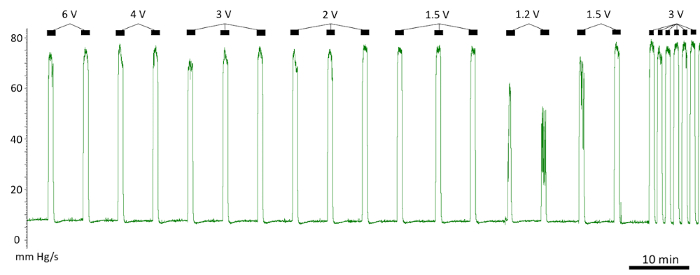
Figure 18. The effect of voltage on pressure response to stimulation. The voltage between 1.5-6 V produced an identical pressure response. The response diminished below 1.5 V. Please click here to view a larger version of this figure.
