The nebulizer system described in protocol section 1 can be constructed from easily-available materials at a low cost. It is intended to be an inset for remote-triggered spraying of the reducing/oxidizing agent inside a bioluminescent reader (Figure 1). Our design allows for the safe operation of the nebulizer within the bioluminescence reader at a 14 cm distance from the lens. No fogging or blurring of the lens was observed during the operation. We selected the commercially-available chemiluminescent agent [Ru(bpy)3]Cl2 for the development of our method based on its low price, stability in aqueous solution, well-described redox behavior, and chemiluminescent properties (Figure 2)19. The minimal detectable signal can be determined as described in protocol section 2 by oxidizing one drop of [Ru(bpy)3]Cl2 (100 µL, 6.9 pmol- 347 nmol in H2O) with (NH4)2Ce(NO3)6 (100 µL, 25 mM) on a microscope slide. Then, by using the nebulizer and spraying on a solution of triethylamine (1:3 in water/ethanol), the chemiluminescent signal is triggered. In our case, the minimal detectable signal was determined to be 6.9 pmol/cm2 (Figure 3). It is conceivable, though, that optimized reaction conditions, camera sensitivities, shutter times, volumes, and reagent concentrations might lead to even lower detection thresholds. These reaction conditions can also be used for exploring and testing the chemiluminescence of any given combination of metal complexes, oxidizing agents, and reductants.
Moving to the in vivo experiments in protocol sections 3 and 4, female nude (outbred) mice 5-6 weeks old and NU/J male mice 6-8 weeks old were used. For intravenous injections, amounts of 8-33 nmol of [Ru(bpy)3]Cl2 in 100 µL of PBS per mouse (n = 5) were chosen. The animals were sacrificed 10 min after injection, and the abdominal cavity was exposed. The mice were placed in the bioluminescent reader with the nebulizer pointing towards the tissue of interest (Figure 4). For imaging with intravenously-injected [Ru(bpy)3]Cl2, the chemiluminescent signal was detected predominantly in the kidneys, strongly suggesting renal elimination of the hydrophilic small molecule (Figure 5). Signal-to-noise ratios for mice injected with [Ru(bpy)3]Cl2 versus PBS were 27/1 for the kidney and 21/1 for the liver. For lymph node imaging, 80 nmol of [Ru(bpy)3]Cl2 in 10 µL of PBS were injected subdermally into the hind foot pad of mice (n = 5). Mice were sacrificed 15 min post injection by CO2 asphyxiation. The skin covering both the inner hind legs was removed to expose the muscle, lymph nodes, and lymphatic vessels. Subsequent chemiluminescent visualization of the popliteal lymph nodes led to the observation that lymph nodes containing [Ru(bpy)3]2+ show a 10 ± 4.3-fold higher radiance than untreated ones (167,000 p/(s×cm2×sr) and 17,000 p/(s×cm2×sr); P <0.028) (Figure 6).
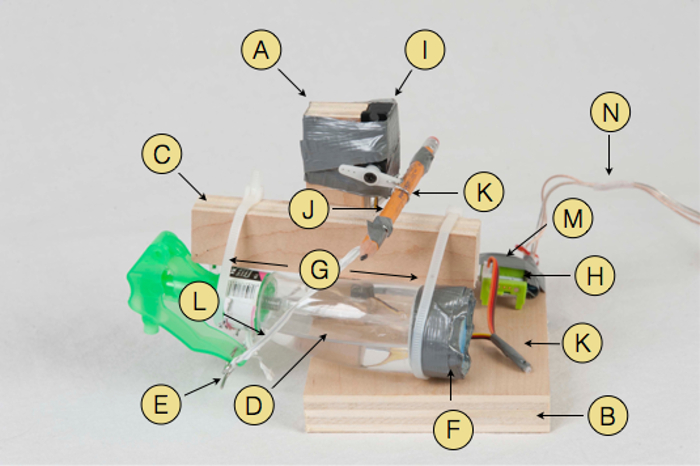
Figure 1: Photograph of the Nebulizer. Parts used: Wooden structure parts (A, B, C), spray bottle (D), bent steel rod (E), duct tape (F), plastic cable ties (G), 011 servo connector part (H), servo motor (I), pencil (J) held by bent paper clip (K), plastic covered wire twist ties (L) w1 wire connector (M) and speaker cable (N) leading to the battery. This figure is based on research originally published in reference19. Please click here to view a larger version of this figure.
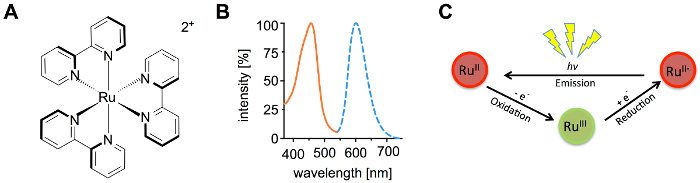
Figure 2. Properties of [Ru(bpy)3]2+. Structure (A) and excitation and emission spectra (B) of [Ru(bpy)3]2+. The oxidation/reduction based chemiluminescent catalytic cycle (C). This figure is based on research originally published in reference19. Please click here to view a larger version of this figure.
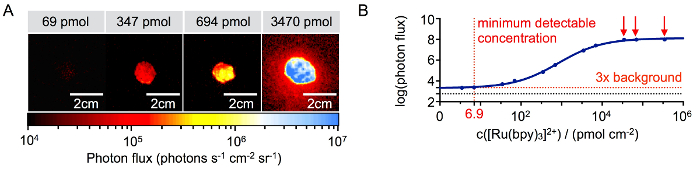
Figure 3: Detection Threshold of [Ru(bpy)3]2+. Representative signal intensities at different concentrations of [Ru(bpy)3]2+ on a microscope slide (A). Imaging signal quantification with detection threshold (red dotted line) and background (black dotted line) (B). This figure is based on research originally published in reference19. Please click here to view a larger version of this figure.
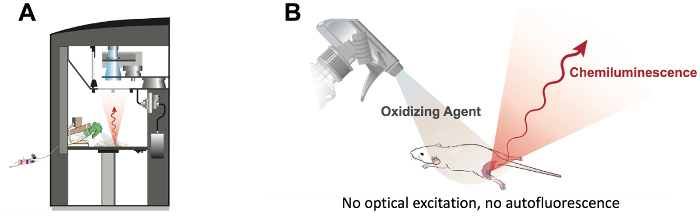
Figure 4: Chemiluminescence Imaging. Schematic drawing of a mouse and a nebulizer positioned in the bioluminescence reader (A) and schematic drawing (B) of the nebulizer spraying on a mouse. This figure is based on research originally published in reference19. Please click here to view a larger version of this figure.
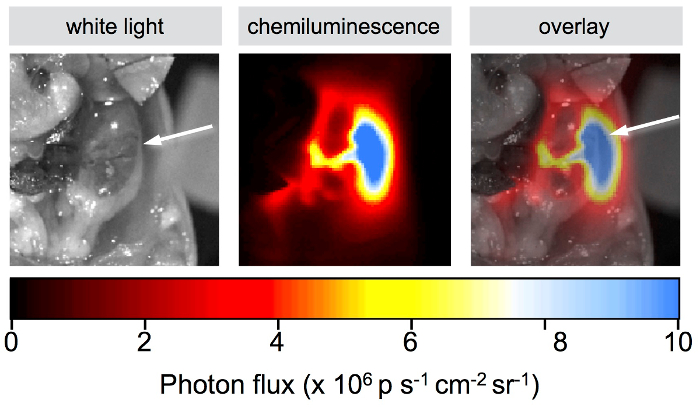
Figure 5: Detection of [Ru(bpy)3]2+ after Systemic Administration. White light, chemiluminescence, and overlay (from left to right). Images of a mouse body cavity that was injected with 33 nmol of [Ru(bpy)3]2+ and sprayed with (NH4)2Ce(NO3)6. The white arrow points towards the right kidney. This figure is based on research originally published in reference19. Please click here to view a larger version of this figure.
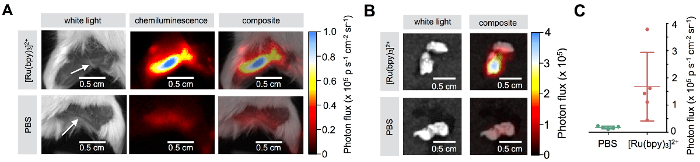
Figure 6: Detection of [Ru(bpy)3]2+ after Subdermal Administration. Popliteal lymph node imaging showing white light, chemiluminescence, and composite pictures for mice injected with [Ru(bpy)3]2+ (top) and PBS (bottom) in the hind limbs; 80 nmol in 10 µL of PBS, imaged 15 min after injection (A). White light and composite images for [Ru(bpy)3]2+ (top) and PBS (bottom)-treated excised popliteal lymph nodes (B). Quantification of chemiluminescent signals for PBS and [Ru(bpy)3]2+-treated lymph nodes (C).The data represents the mean ± SD. This figure is based on research originally published inreference19. Please click here to view a larger version of this figure.
