Ex Vivo Model created to study the wound healing process in the cells’ native microenvironment
To investigate mechanisms involved in regulating wound healing of an epithelium within the cells’ native microenvironment, a clinically relevant ex vivo mock cataract surgery model was created. This model is created from lens tissue which offers many advantages due to its intrinsic properties: 1) the lens is a self-contained organ surrounded by a thick basement membrane called the lens capsule; 2) it is avascular, 3) not innervated and 4) free of associated stroma. Therefore, the repair process examined is limited to cells that are innate to the lens proper. To create this model, lenses are removed from an embryonic (E) day 15 chick embryo (Figure 1A). A small incision is made in the anterior lens capsule and its associated lens epithelial cells through which the lens fiber cell mass is removed by hydro-elution, a classic cataract procedure that creates a physiologically relevant wounding (Figure 1A). The lens epithelium, which is present as a continuous monolayer of cells along the anterior and equatorial aspects of the lens capsule surrounding the fiber cell mass, along with its endogenous population of vimentin-rich mesenchymal repair cell progenitors1, remain in the lens during the extraction of fiber cells (Figure 1A). Following removal of the fiber cell mass, five cuts are made in the anterior aspect of the lens capsule and the epithelium flattened cell-side up, facing the medium. This procedure enables imaging of the response of the injured epithelium by various microscopic approaches, including time-lapse microscopy (Video 1). These additional cuts in the anterior lens capsule create a star-shape explant of the wounded lens with the circular wound created by removing the fiber cell mass in the center of the explant (Figure 1B). Post-cataract surgery and flattening of the tissue, the wounded epithelium is located in the points of the star, which is referred to as the Original Attachment Zone (OAZ) (Figure 1A, B).
The removal of the fiber cell mass from its attachment site on the posterior lens capsule creates a highly reproducible wound area on the basement membrane, surrounded by the wounded epithelium (Figure 1B, C). The exposed edge of the lens equatorial epithelium, just adjacent to where the fiber cells were attached, is the leading edge of the wound. Immediately following injury, a subpopulation of vimentin-rich mesenchymal repair cells is activated and migrates to the wound edge of the epithelium1. The lens epithelium, with these mesenchymal repair cells at their leading edge, rapidly moves onto the cell-free region of the endogenous basement membrane capsule, the Central Migration Zone (CMZ), to begin healing the wound. Lens epithelial cells move collectively, as a sheet, into the CMZ led by the mesenchymal leader cells1, which extend protrusions along the substrate and direct the wound healing process (Figure 1D, Video 1). Wound healing progresses, covering a significant area of the wound (67%) by day 1 in culture (Figure 1C), and is typically completed within 3 days in culture (Figure 1B, C).
A clear physical distinction can be made between the OAZ and CMZ regions as early as day 1, which is demarcated as a crease or wrinkle between these two zones (Figure 2A, arrow). This phenomenon provides a guideline by which to separate these areas at any point during the wound healing process. Using a fine tipped forceps, the cultures can be micro-dissected to separate the OAZ and CMZ regions in order to analyze molecular differences between these distinct zones (Figure 2B). This is a powerful approach that has been used to identify migration-specific changes associated with wound-repair. Previously, it was found that there is an increase in Focal Adhesion Kinase (FAK) activation in the ex vivo wounded cultures during the wound healing process5. FAK has a well-established role in cell migration26-29. The ability to enrich for the OAZ vs. CMZ now made it possible to examine whether this increase in FAK activation is specific to the migration-specific CMZ region. For this study, the OAZ and CMZ regions were separated on day 1 – 3 (throughout the wound healing process) and analyzed for biochemical changes in FAK activation (FAK pY397). The results demonstrated that the increase in FAK activation was associated with the migration-specific CMZ region (Figure 2C). The ex vivo model system described here provides a unique and invaluable opportunity in which to investigate the molecular programs involved in coordinating the wound repair process.
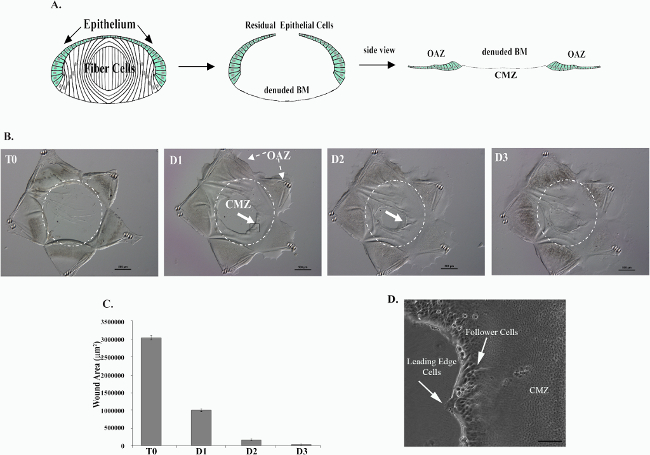
Figure 1. Creation of an ex vivo model in which to study the wound healing process within the cells’ native microenvironment in response to a physiological wounding. Mock cataract surgery was performed on E15 chick lenses. The lens fiber cell mass (white) is removed through an incision in the anterior capsule by hydro-elution. This process leaves behind epithelial cells (green) that remain tightly adherent to the lens capsule and a cell-denuded basement membrane (BM) onto which cells will migrate to heal the wound (A). Five cuts are made to the epithelium to flatten out and create a star shaped ex vivo culture (B). The residual lens epithelial cells that fill the points of the star are referred to as the Original Attachment Zone (OAZ) (A, B). The denuded BM onto which cells will migrate is referred to as the Central Migration Zone (CMZ) (A, B). Immediately in response to injury, cells begin to move into the CMZ region on the cell-denuded BM (B). The open wound area is quantified over time in (C). Wound healing is typically completed by D3 in culture (B, C). In (B, C) T0 denotes time of wounding, D1-3 denotes Days 1-3. Within the CMZ, two populations of cells can be distinguished, the lens epithelial cells and the mesenchymal leader cells that localize to the wound edge, extending protrusions along the substrate (D). This figure is reprinted from Menko et al 23.Please click here to view a larger version of this figure.
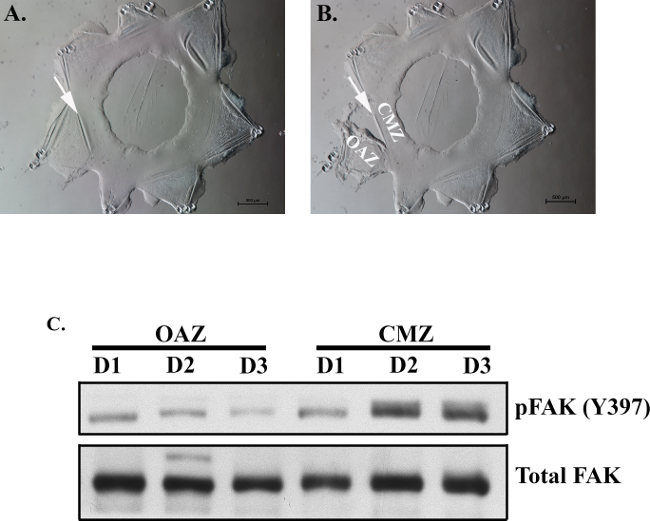
Figure 2. Separation of OAZ and CMZ regions to identify migration-specific changes associated with wound healing. By day 1, OAZ and CMZ regions can be distinguished from one another by a crease (arrow), which can be used as a guide to separate these zones (A). At this crease, fine tipped forceps can be used to grip the edge of the OAZ/CMZ line. The culture can be separated along this line allowing isolation of the OAZ and CMZ regions (B). Micro-dissection of the OAZ and CMZ daily, from day 1 (D1) – day 3 (D3) was performed to determine if migration-specific changes in FAK activation occur in the region of wound repair. Lysates from each region were examined by Western blot analysis for either FAK activation (pFAK Y397) or Total FAK expression (C). While little change in total FAK levels was observed, an increase in FAK activation was associated with the migration-specific CMZ region (C).
Video 1. Wound healing in the ex vivo mock cataract surgery model is followed by time-lapse microscopy from time 0 after injury through to day 3. Wound closure is viewed from the center of the wound area.
