Directed Differentiation of Human iPSCs into iHeps
When reaching 70% confluence, human iPSCs are differentiated into iHeps with a 3-step protocol16 (Figure 1 upper panel). After 3 days of endoderm differentiation, iPSC colonies become loosened and spread to full confluence (Figure 1 lower panel). Then, with 2nd stage medium, hepatoblasts appear and proliferate. These cells are crowded but show clear edges at this stage (day 7, Figure 1 lower panel). After 17 days of differentiation, polarized iHeps with typical hexagon morphology appear (Figure 1 lower panel). These iHeps express pHH markers, including AAT and ALB (Figure 2A). Moreover, the ratio of ASGPR+ iHeps should be relatively high, as measured by flow cytometry (Figure 2B)15.
Generation of a FH In Vivo Disease Model Using FH iHeps
To help LRG mice develop hypercholesterolemia, we feed them with a HFHC diet 7 days prior to engraftment (day -7). On the day of engraftment (day 0), LRG mice display around 3-fold plasma LDL-C level (around 600 mg/dL, Figure 3B). Day 15–17 iHeps are engrafted into LRG mice via intrasplenic injection; these iHeps soon reside in the liver parenchyma and proliferate there (Figure 3A). At the end-point, livers of these chimeric mice are collected and fixed, then stained with hALB and hNA, both of which should show clear proof of iHep-mediated liver repopulation in LRG mouse liver based on staining for hALB and hNA (Figure 4A-E). In our hands, both LDLR +/- and FH iHeps could reduce plasma LDL-C level significantly 21 days post-engraftment (Figure 4F). At this point, FH human liver chimeric mice can be used to test therapies for FH.
Validation of FH Human Liver Chimeric Mouse Model Using Available Drugs
To validate our model, we used 2 well-known LDL-C lowering drugs, simvastatin and PCSK9 antibodies (Figure 5A). Our data demonstrate that 21 days after treatment, PCSK9 antibodies have a stronger ability for LDL-lowering and EDV than simvastatin in FH chimeric mice (Figure 5B-D). Notably, the observed percentage reduction of plasma LDL-C with PCSK9 antibodies in FH chimeric mice is similar to that reported in clinical trials4. These results demonstrate the potential utility of LRG chimeric mice engrafted with FH iHeps for preclinical testing of novel drugs for FH.
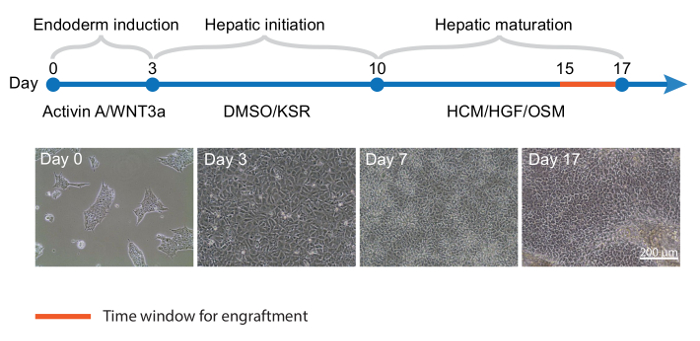
Figure 1: Directed Differentiation of Human iPSCs into iHeps.Top panel, Timeline for iPSC differentiation into iHeps; key cytokines and media are shown for each stage. (Lower panel) Representative phase contrast images of different time points of iHep differentiation. KSR: knockout serum replacement; HCM: hepatocytes culture medium; HGF: hepatocyte growth factor; OSM: oncostatin M. Please click here to view a larger version of this figure.
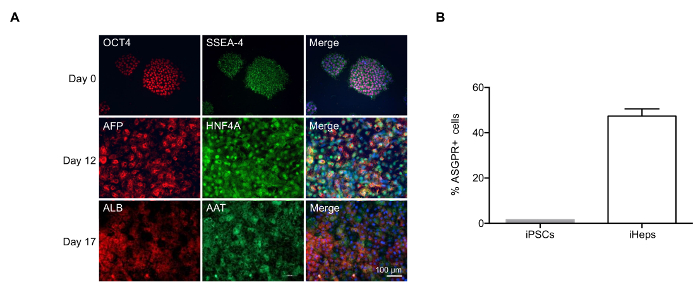
Figure 2: Characterization of iHeps Produced with Modified Differentiation Protocol. (A) Immunofluorescence of iHeps at various stages of differentiation. Nuclei are stained in blue in the merged compositions. (B) Bar graph shows the percentage of ASGPR+ iHeps derived obtained at day 17, as measured by flow cytometry. Samples were measured in 3 independent experiments; mean values are shown and error bars indicate standard deviation (SD). Please click here to view a larger version of this figure.
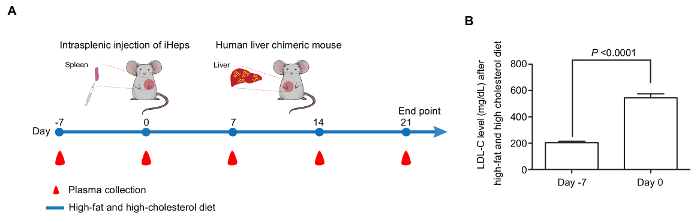
Figure 3: Generation of a FH In Vivo Disease Model with iHeps. (A) Time line for the generation of human liver chimeric mice by intrasplenic injection of FH iHeps into LRG mice. (B) Bar graph shows that feeding LRG mice with HFHC diet leads to significantly increased LDL-C level (n = 10). P values are indicated on the figure and were obtained using an unpaired t-test; mean values are shown and error bars indicate standard error of the mean (SEM). Panel B is modified from Figure 3I of our previous report15. Please click here to view a larger version of this figure.
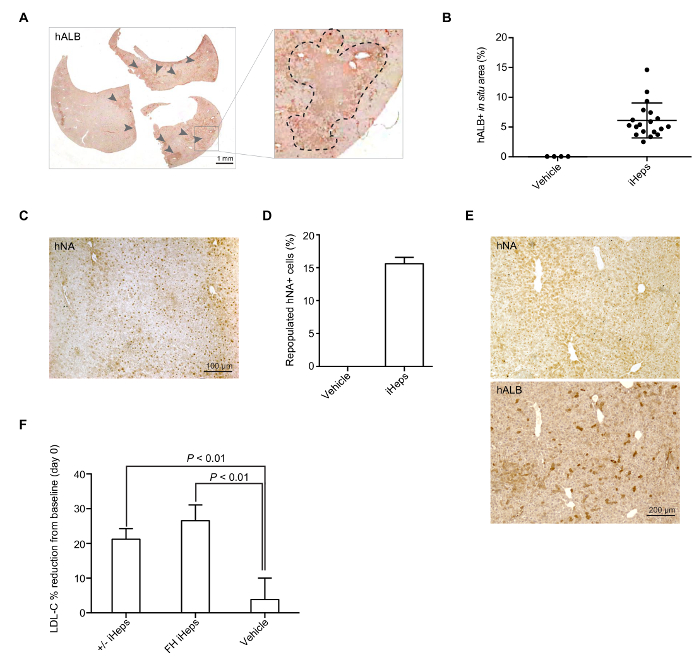
Figure 4: iHep Mediated Repopulation of LRG Mice Liver. (A) Representative whole section-scanned image of hALB staining in a mouse liver repopulated with LDLR +/- iHeps. Arrows indicate clusters of human iHeps engrafted into the mouse liver; zoomed sections are shown in the right panel. (B) Scatter plot graph shows the percentage of repopulated hALB+ corresponding to iHep-containing areas in a mouse liver (from different donor iPSCs), calculation was based on whole section-scanned images (n = 19). Mean values are shown and error bars indicate SD. (C) Representative images of immunohistochemical staining for hNA in a mouse liver with engrafted FH iHeps. (D) Bar graph shows the percentage of repopulated hNA+ iHeps (from different donor iPSCs) in LRG mouse livers (n = 3). Mean values are shown and error bars indicate SD. (E) hALB and hNA staining on two consecutive sections of a mouse liver repopulated with wild type iHeps. (F) Bar graph shows the percentage of plasma LDL-C reduction from baseline at day 21 post-engraftment; n = 5 for LDLR +/- iHeps and n = 6 for FH iHeps and the vehicle. P values are indicated on the figure and were obtained using an unpaired t-test; mean values are shown error bars indicate SEM. Panels B, D, and E are modified from Figure 3G-3I of our previous report15. Please click here to view a larger version of this figure.
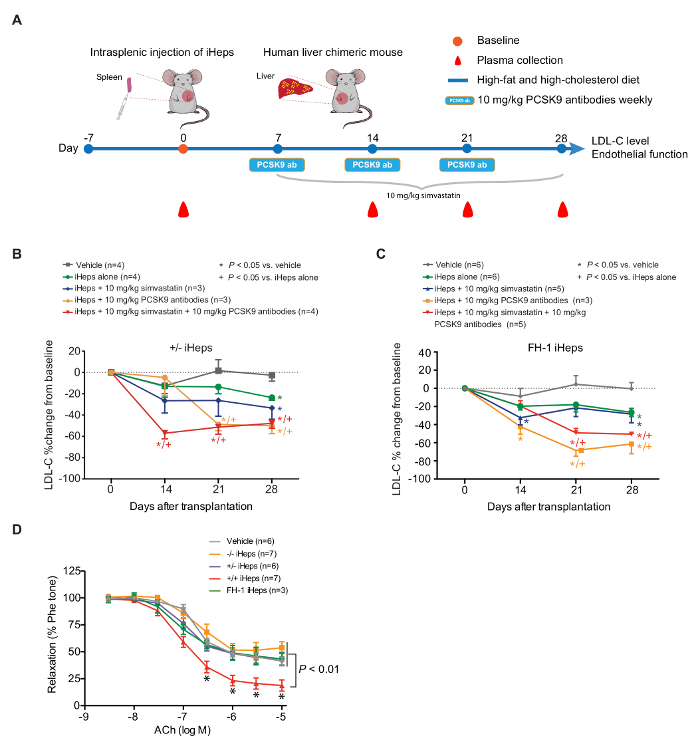
Figure 5: PCSK9 Antibodies Show Stronger LDL Lowering Ability than Simvastatin in Human Liver Chimeric LRG Mice. (A) schematic view of the in vivo drug testing approach using FH human liver chimeric mice. (B and C) Percentage change of plasma LDL-C from baseline at days 14, 21, and 28 in FH chimeric mice fed with HFHC diet and treated with the indicated drugs; n indicates number of mice. P values were obtained using a Kruskal-Wallis test; mean values are shown and error bars indicate SEM. (D) EDV in response to increasing concentrations of ACh. P values are indicated on the figure for indicated concentration. P values were obtained using two-way ANOVA adjusted with Dunnett's multiple comparison; error bars indicate SEM. Figure 5 is modified from Figure 4A–4C and Figure 5A of our previous report15. Please click here to view a larger version of this figure.
