Troubleshooting FoCUS Image Acquisition: Patient Positioning, Transducer Manipulation, and Image Optimization
Summary
Here, we present a protocol to allow providers to perform focused cardiac ultrasound (FoCUS) in the clinical environment. We describe methods of transducer manipulation, review common pitfalls of transducer movements, and suggest tips to optimize phased array transducer use.
Abstract
Focused cardiac ultrasound (FoCUS) is a limited, clinician-performed application of echocardiography to add real-time information to patient care. These bedside exams are problem oriented, rapidly and repeatedly performed, and largely qualitative in nature. Competency in FoCUS includes mastery of the stereotactic and psychomotor skills required for transducer manipulation and image acquisition. Competency also requires the ability to optimize the setup, troubleshoot image acquisition, and understand the sonographic limitations because of complex clinical environments and patient pathology. This article presents concepts for successful, high-quality two-dimensional (B-mode) image acquisition in FoCUS.
Concepts of high-quality image acquisition can be applied to all established sonographic windows of the FoCUS exam: the parasternal long-axis (PLAX), parasternal short-axis (PSAX), apical four chamber (A4C), subcostal fourchamber (SC4C), and the inferior vena cava (IVC). The apical five-chamber (A5C) and subcostal short-axis (SCSA) views are mentioned, but are not discussed in-depth. A pragmatic figure illustrating the movements of the phased array transducer is also provided to serve as a cognitive aid during FoCUS image acquisition.
Introduction
Focused cardiac ultrasound (FoCUS) is a limited, clinician-performed application of echocardiography that provides immediate anatomic, physiologic, and functional information to patient care. These exams, consisting of five classic views, are problem oriented, performed in real time at the bedside, and do not replace comprehensive echocardiography exams1,2. Given the focused nature of these exams, they are often repeatedly performed when clinical status changes or serial monitoring is required. It is important to have standardized training and obtain adequate images of all five views, when possible, as some views may provide limited information depending on the individual patient and pathology.
The use of FoCUS is rapidly expanding. Many clinical landscapes, such as perioperative anesthesiology, critical care and emergency medicine1,2,3, now routinely employ FoCUS. Inpatient medical wards and outpatient clinical care settings are also adopting this tool to enhance clinical practice4,5,6. As a result, several societal bodies, such as the American Society of Echocardiography, the Society of Critical Care Medicine, and the American College of Emergency Physicians, have published guidelines and recommendations for FoCUS competency and scope of practice7,8,9. While these guidelines and recommendations are not codified, much of the content is consistent and influences FoCUS training curricula10.
Beyond didactics and image interpretation, competency in FoCUS includes mastery of stereotactic and psychomotor skill sets. Stereotactic skill refers to the accurate positioning of ultrasound transducers on the body, based on three-dimensional anatomic features. Psychomotor skill describes the relationship between cognitive function and physical movement that influences coordination, dexterity, and manipulation. Expanding knowledge and awareness about these skills supports FoCUS trainee development.
This article presents concepts for high-quality image acquisition in FoCUS, with both pragmatic considerations and attention to stereotactic and psychomotor skill sets. Specifically, it discusses optimal patient positioning, transducer manipulation, and suggests tips to optimize phased array transducer use. Finally, it examines image optimization for 2-dimensional (B-mode or 2-D mode) and motion modes (M-mode).
Protocol
This material is the authors' original work, which has not been previously published elsewhere. The protocol described is for clinical use and not research purposes. De-identified images were obtained from a volunteer model in a non-clinical environment. The authors did not seek a formal "Not Regulated" determination from the IRB in accordance with institutional policy, as the activity falls outside of the Common Rule and FDA definitions of human subject research.
1. The transducer
- Use the phased array transducer. This is a 4-12 MHz transducer that penetrates deep into the thoracic space, due to its low frequency compared to other ultrasound transducers.
- Select the phased array transducer using the Exam button on the machine and selecting the cardiac exam or equivalent available exam.
- Practice with transducers from various vendors to gain experience and refine one's cognitive skill set for transducer manipulation.
- Practice transducer manipulation with both hands to develop ambidexterity, which may be required when working in limited clinical environments.
- Anchor the dominant hand while holding the ultrasound transducer on the patient, with the fat pad of the medial aspect of the hand.
NOTE: This provides additional stability and reduces error caused by large movements. Holding the transducer by the base, without anchoring, results in unintended movements, preventing the ability to maintain the image axis and orientation. - Use two hands for transducer manipulation to improve the ultra-fine adjustments often required for optimal views. Place the dominant hand on the base of the transducer with the non-dominant hand on the tail of the transducer, providing additional stability and guided movement.
2. Patient positioning
- Obtain the PLAX, PSAX, A4C, SC4C, and IVC views in the supine position.
- Instruct the patient to extend their left arm above their head and lie on their left side, and obtain images in this position if they are unable to be obtained in the supine position.
NOTE: This results in expansion of the intercostal spaces for larger imaging windows.- Place a wedge or blanket roll behind the patient's right upper torso if the patient cannot easily rotate to 45°, or reposition their limbs. Postoperative and intensive care unit patients often need support to maintain appropriate positioning for FoCUS examination.
- Drape the breast as desired by the patient, and make sure that the patient is aware of where the transducer will be placed before beginning the exam.
- Manipulate the breast tissue to allow for optimal image acquisition.
- If able, instruct the patient to assist moving the breast tissue with their right hand.
- Discuss the appropriateness of removal or relocation of monitors beforehand with bedside nurses and other relevant providers.
- Do not alter or remove tubes, lines, or drains for imaging purposes. Discuss the duration of the devices with the relevant providers and consider reimaging the patient following their removal.
3. Transducer manipulation
- Appreciate and understand the definitions of transducer movements to allow for optimal image acquisition, and provide consistent terminology for communication between providers, especially during teaching (Figure 1 and Table 1).
4. 2-D image optimization
- Adjust the depth (approximately 12-16 cm, depending on view) to see the structure of interest.
- Adjust the gain to optimize the brightness of the image.
- Adjust the focus to the depth of the structure of interest in order to improve resolution.
5. Motion mode (M-mode)
- Use M-mode to display a single scan line (wherever the cursor is placed) of the B-mode image (Y-axis) against time (X-axis).
NOTE: This mode can help operators understand the dynamic relationship of different structures over time and is useful in many different assessments, including IVC size and variability and E-point septal separation (EPSS). - Use the button with the letter "M" on it to turn on M-mode.
NOTE: M-mode will be an on/off button unique to each machine.
6. Parasternal long axis (PLAX)
NOTE: The PLAX refers to obtaining an image that is along the long axis of the heart (Figure 2).
- Place the patient in the supine position. If there is difficulty obtaining the PLAX image, place the patient on their left side and extend their arm above their head, if possible.
- Place the transducer at an oblique angle between the third and fifth intercostal space of the left parasternal region, with the transducer marker pointing to the patient's right shoulder.
- Visualize the right ventricle, left ventricle, left atrium, mitral valve, left ventricular outflow tract, aortic valve, and descending thoracic aorta in this image.
- Visualize the mitral valve and aortic valve opening and closing together, to ensure that the image is not foreshortened. Foreshortening is where the ultrasound plane does not cut through the true apex of the structure, changing the perceived image.
- 2-D image optimization
- Start with an initial depth of approximately 15-20 cm. Adjust the depth so that the tip of the mitral valve is in the center of the image, and the descending thoracic aorta (deep to the left atrium) is visible.
- Adjust the gain to maximize the visibility of the myocardium and mitral valve.
- Move the focus to the region of interest, most focused at the depth of the mitral valve.
- Use M-mode for EPSS or fractional shortening.
7. Parasternal short axis (PSAX; Figure 3)
- Place the patient in the same positioning for the PSAX as used for the PLAX.
- Place the transducer approximately 90° relative to the transducer in the PLAX.
- Obtain an optimal PLAX and rotate the transducer slowly in a clockwise fashion without lifting the transducer from the patient's chest, until the transducer is obliquely angled across the third to fifth intercostal space of the parasternal region, with the transducer marker pointing to the patient's left shoulder.
NOTE: Over-rotation beyond 90° can lead to interventricular septal flattening, and falsely appear as right ventricular volume or pressure overload. - Tilt the transducer until the mid-papillary muscles are visualized for the FoCUS assessment.
NOTE: The papillary muscles should move in synchrony with the left ventricle wall. If the papillary muscles appear to be bouncing or fluttering independent of the left ventricular wall, it may signify that the image is capturing the mitral valve leaflet as a result of being off axis. - Tilt the transducer toward the base of the heart, to visualize the bi-leaflet mitral valve initially followed by the tri-leaflet aortic valve.
- Obtain an optimal PLAX and rotate the transducer slowly in a clockwise fashion without lifting the transducer from the patient's chest, until the transducer is obliquely angled across the third to fifth intercostal space of the parasternal region, with the transducer marker pointing to the patient's left shoulder.
- 2-D image optimization
- Start with a deeper image (approximately 16 cm) to identify any pleural effusion.
- Adjust the depth to include the full depth of the left ventricle and a few centimeters beyond, to ensure that a pericardial effusion would be fully visualized.
- Adjust the gain to maximize visualization of the septum and papillary muscles.
- Adjust the focus to the papillary muscles.
8. Apical four chamber view (A4C; Figure 4)
NOTE: Images in patients with chronic obstructive pulmonary disease (COPD), and otherwise inflamed thoracic cavities, are obtained more medially, and images in patients with left ventricular hypertrophy (LVH) or heart failure with reduced ejection fraction (HFrEF) have their view more lateral.
- Position the patient with their left arm extended above their head and lying on their left side. If there is significant artifact present, have the patient exhale and hold their breath to minimize pulmonary artifact.
- Position the transducer in the fourth through sixth intercostal space along the left anterior axillary line (inferolateral to the left pectoral muscle), with the transducer marker pointed toward the left axilla. Move the transducer lateral, medial, or caudal, as needed to obtain an optimal A4C view.
- Lift the breast tissue and push superior along the inframammary fold as needed.
- If the left ventricular apex is not fully visualized, move the transducer lateral while orienting the transducer toward the right shoulder.
- Position the marker on the phased array transducer between the two and three o'clock positions. In the normal heart, the apex of the left ventricle is at the top and center of the sector, the right ventricle is triangular and smaller, and the myocardium should be uniform from the apex to the atrioventricular valves. If this is not the case, the image may be foreshortened, and should be optimized and acquired from a lower intercostal space.
- Tilt the transducer cephalad approximately 60°, so that the A4C view can capture an A4C cardiac image that includes both atria, ventricles, the interventricular septum, and the lateral portions of the tricuspid and mitral annuli. The aortic valve and left ventricular outflow tract should not be present in an A4C view, and are only present in an apical five chamber view.
- Visualize the mitral valve, the tricuspid valves, and the interventricular septum on the A4C image. If both valves and the interventricular septum are not visualized, the image should be further optimized.
- Slide the transducer up or down a rib space and tilt the base of the transducer down (cranially) to improve the image of the valves. If the base of the transducer is tilted too far down (cranially), an apical five chamber view, including the aortic valve, will appear, and the transducer should be tilted back up (caudally) to optimize the A4C view. If the base of the transducer is tilted too far up (caudally), the coronary sinus will appear, and the transducer should be tilted back down (cranially).
- Rotate the base of the transducer toward the patient's midline to optimize the interventricular septum position, which should be present vertical in the center of the image. Minimal rotation should be required. If over-rotated, a two chamber view will be observed.
- 2-D image optimization
- Increase the depth to include both atria at the image's deepest point, in addition to accommodating the left and right ventricular free walls (approximately an initial depth of 20 cm).
- Adjust the gain to maximize visibility, often resulting in increased echogenicity, of the myocardium, the mitral valvular annulus, and the tricuspid valvular annulus.
- Adjust the focus to the depth of the valvular annuli (the tricuspid annulus is most commonly used). This depth will also be appropriate when transitioning to an apical five view, if desired.
9. Subcostal four chamber view (SC4C; Figure 5)
- Position the patient supine for the subcostal four chamber view. Flex the patient's knees, and support them to maintain the flexed position, to reduce the abdominal muscle tone for easier transducer compression.
- Place the transducer nearly flat on the patient's subxiphoid abdomen, with the operator hand on top of the transducer providing cephalad pressure. Find the liver, and then drop the transducer to a shallower angle (often less than 30°) against the subxiphoid portion of the patient's abdomen in a cephalad fashion, with the transducer marker to the patient's left side, approximately pointing to three o'clock. Include the liver in the image so that it can be utilized as an acoustic window to obtain this image.
- Hold the lateral aspects of the transducer with the fingers, not underneath the transducer, to flatten the transducer appropriately. Use the index finger to provide downward pressure.
- 2-D image optimization
- Start with an initial depth of 18-24 cm. Adjust the depth to include the liver as a sonographic window for the ultrasound. The optimal depth varies from patient to patient based on patient body habitus and liver size.
- Decrease the gain, as the liver often provides a good medium to transmit sound waves.
- Increase the focal points to focus on the cardiac structures of interest below the liver.
- Instruct non-intubated patients to perform an inspiratory hold, as this often increases the quality of the image.
10. Inferior vena cava (IVC; Figure 6)
- Position the patient supine for the IVC view.
- Begin with the subcostal view, then rotate the transducer counterclockwise until confluence of the right atrium and IVC is appreciated, and the transducer is placed longitudinally in the upper abdomen, to the right of the patient's midline. Optimize the image by tilting the transducer until the IVC is fully visualized, and then by rocking the transducer cephalad until the confluence of the IVC and the right atrium is fully visualized. Adjust the transducer (most frequently with minimal rotation) until the IVC is visualized across the entire screen.
- Visualize the right atrium, IVC, liver, and hepatic vein in an optimal view.
- Do not confuse the IVC with the aorta. The aorta is left lateral of the IVC and will not touch the liver. The IVC will always touch the liver, and is often surrounded by liver on both sides.
- Appreciate that hepatic veins can often be seen coming into the IVC, providing another way to prove that the structure being imaged is the IVC.
- Use pulse wave velocity to visualize the venous (vs. arterial) waveform, and confirm the vessel being imaged is the IVC and not the aorta.
- Measure IVC diameters at midline and mid-expiration. Do not measure the diameter of the IVC to the side which could underestimate the diameter of the IVC.
- 2-D image optimization
- Minimize the depth to only include the IVC. Do not include the spine in the image.
- Adjust the gain to be the same as for the subcostal view.
- Adjust the focus to the depth of the IVC.
- Place the cursor 1-3 cm from the confluence of the IVC and the right atrium, and apply M-mode to evaluate respiratory variation of the IVC.
Representative Results
Representative images obtained from the focused cardiac ultrasound protocol presented above are presented in Figure 2, Figure 3, Figure 4, Figure 5, and Figure 6, demonstrating the feasibility of the technique described. These images were captured with the phased array 5-1 MHz transducer. The parasternal long axis (PLAX) image obtained from protocol section 7 is displayed in Figure 2. The parasternal short axis (PSAX) image obtained from protocol section 8 is displayed in Figure 3. The apical four chamber (A4C) image obtained from protocol section 9 is displayed in Figure 4. The subcostal four chamber (SC4C) image obtained from protocol section 10 is displayed in Figure 5. The inferior vena cava (IVC) image obtained from protocol section 11 is displayed in Figure 6. The representative images were obtained from a volunteer model in a non-clinical environment, who was not undergoing clinical care at the time the images were obtained.
| Term | Why | Transducer Movement | ||||
| Slide | Looking for the best sonographic window, following a structure, or moving to a different region of the body | Move the entire transducer in a specific direction without rotation or changes in transducer angle, orientation, or compression. Some literature specifies that sliding is movement along the long axis of the transducer while sweeping is movement along the short axis. | ||||
| Tilt | This allows for visualization of multiple cross-sectional images of various cardiac structures | Change the angle of the transducer, in the short axis, relative to the patient in a side-to-side fashion. | ||||
| Rotate | Most commonly used to switch between the long and short axis – in FoCUS this can be used to go from parasternal long axis to parasternal short axis. | Turn the transducer in a clockwise or counterclockwise direction relative to its central axis. The position and angle between the transducer and patient is maintained. | ||||
| Rock | Rocking allows the provider to center the area of interest, often referred to as in-plane motion | Change the angle of the transducer in the long axis relative to the patient. | ||||
Table 1: Transducer manipulation.
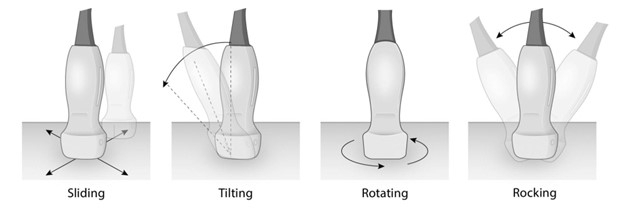
Figure 1: Phased array transducer manipulation/movement (sliding, tilting, rotating, rocking).
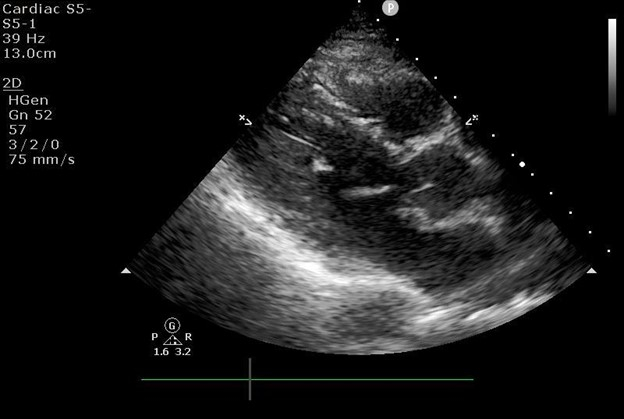
Figure 2: Focused cardiac ultrasound parasternal long axis image.
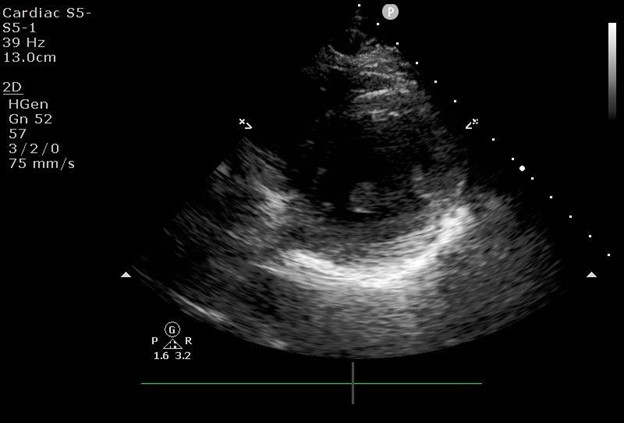
Figure 3: Focused cardiac ultrasound parasternal short axis image.
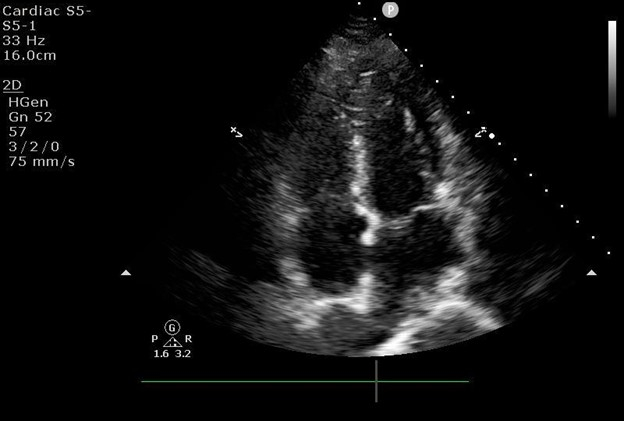
Figure 4: Focused cardiac ultrasound apical four chamber image.
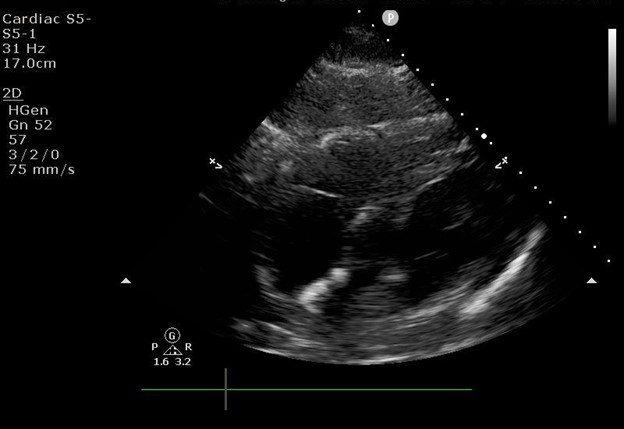
Figure 5: Focused cardiac ultrasound subcostal four chamber image.
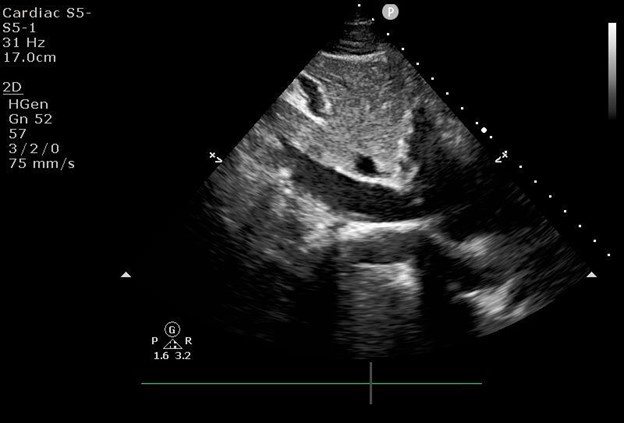
Figure 6: Focused cardiac ultrasound inferior vena cava image.
Discussion
The aim of this publication is to provide practical recommendations and best practices to achieve optimal FoCUS images in challenging clinical environments. Formal ultrasound seminars, clinical experience, and observations of learners during hands-on teaching have given insight into pitfalls and less optimal tendencies. As a result, many factors that influence the stereotactic and psychomotor skills have become apparent. Although this material is described in relation to FoCUS exams, many of the principles can be applied to other point of care ultrasound exams and ultrasound transducer types. In addition to impacting learners, instructors can incorporate these concepts into their teaching material and methodology.
There are many basic principles of ultrasonography that must be considered to acquire optimal images. Appropriate transducer selection is critical for optimal image acquisition. The phased array transducer, a 4-12 MHz transducer that penetrates deep into the thoracic space, should be used for the FoCUS exam. Use of the phased array transducer requires delicate and fine adjustments via the hand to optimize an image. Learners often overcompensate adjustments by rapidly moving the hand or transducer. One must appreciate that transducer movements at the skin are small but associated with longer arc length movements imposed on deeper anatomical structures.
To develop expertise in FoCUS, providers should practice with both hands to develop ambidexterity, and practice with transducers from various vendors to refine their cognitive skills for transducer manipulation. Depending on the vendor and device specification, ultrasound transducers vary in form factor, overall weight, weight distribution, heat generation, and connectivity (cord vs. cordless). This can impact the user experience, such as an increased need for a coupling agent, the cadence of transducer movement between windows, and fine image adjustments. With the development of capacitive micromachined ultrasound transducers, a universal transducer may have a form factor distinct from traditional phased array transducers, that provide users with the desired frequency range setting.
Patient positioning facilitates optimal imaging in patients with initially challenging images. The FoCUS exam is typically performed in the supine position, however the PLAX, PSAX, and A4C can be further optimized by instructing the patient to extend their left arm above their head and lie on their left side. Extensive breast soft tissue, previous thoracic operations, and devices can further inhibit optimal image acquisition. If patient comfort and ability allow, the patient can manipulate their breast, or the non-dominant hand of the scanner can be used to displace the breast tissue. Patients who have had a mastectomy or thoracotomy may have pain with transducer application and bandages or devices that interfere. Breast implants may be encountered, and are visualized as large hypoechoic spaces on imaging. Imaging through bandages and around devices often results in off-axis images, artifact, or void images, and is not recommended. Alternative imaging modalities should be considered.
Ultrasound machine positioning allows for maximal ease and ability to acquire optimal images. By placing the stand-alone upright ultrasound machine on the same side of the patient as the provider, the provider can scan with one hand while performing knobology for image optimization with the other hand. A right-handed provider generally stands on the right side of the patient, with the ultrasound machine on the same side, so that they can scan with their right hand while manipulating the settings with their left hand. A left-handed provider generally stands on the left side of the patient, with the ultrasound machine on the same side, so that they can scan with their left hand while manipulating the settings on the ultrasound machine with their right hand. Providers should become facile with transducer manipulation using both hands, as the clinical environment may dictate the available space.
To fully utilize the imaging abilities of the ultrasound machine, providers must be able to effectively optimize image depth, gain, and focus in real time. Depth determines how deep the ultrasound beams penetrate, and is dependent on the transducer frequency. Depth is a function that is adjusted with a button on the ultrasound machine being used, and is in a different position on each machine. Only the amount of depth necessary to see the structure of interest should be used. Inadequate depth fails to capture the desired structures. Excess depth reduces the frame rate and thus image quality. Reducing the image depth and width improves frame rate. Quantifiable measurements of depth are present along the right side of the screen, and can be used as an estimate for the depth or size of structures. The starting depth is provided for each view, but the optimal depth varies from patient to patient depending on body habitus and anatomical variation.
The gain optimizes the brightness of the image; it increases or decreases the amplitude of the returning ultrasound signals, which affects the brightness of what is visualized on the screen (brightness mode, or B-mode). Under-gained and over-gained are terms used to describe images that are too dark and bright, respectively. Under-gained images reduce the ability to visualize relevant structures, whereas over-gained images potentiate artifacts. All ultrasound machines can adjust (increase or decrease) the gain of the entire image uniformly, while some allow the gain at different depths to be adjusted individually, termed time gain compensation (TGC). The gain can be adjusted on the machine via a turn knob, button, or lever, depending on the machine manufacturer.
TGC allows the gain to be adjusted individually at different depths. This is most frequently accomplished through a column of knobs that can be adjusted from side-to-side. The top rows of TGC knobs adjust the regions of the image with less depth (the near field), while the bottom rows of knobs adjust the regions with the greatest depth (the far field). Some machines simplify the available knobs to "near field" and "far field" to allow for the adjustment of the top (shallowest half) and bottom (deepest half) of the image, respectively. TGC is adjusted on each machine differently, depending on how the manufacturer set up the knobs. It can be a set of levers corresponding to the depth of the field, or a set of three slides for "near", "middle", and "far" field.
The focus, otherwise known as the focal zone, concentrates the ultrasound waves at a specific depth, and is the location along the ultrasound beam that maximizes the lateral resolution. The focal point setting adjusts the focal zone (frequently superimposed on the depth marking) to be aligned at the depth corresponding with the image of interest. The focal point or focal zone is labeled on each machine, and is able to be adjusted up or down by the provider performing the scan.
The progression of FoCUS sonographic windows (sections 8-12) is consistent with the American Society of Echocardiography exam sequence11, and when time permits, following this sequence consistently is recommended. A standard exam sequence ensures unsuspected findings are not missed and builds a repertoire of consistency in exam content and build competency. Furthermore, serial exams for comparison can be performed before and after an intervention, such as a fluid bolus or initiation of vasoactive medications, to assess for intervention effect12.
Additional ultrasound modalities, such as color doppler and pulse wave (PW) doppler, augment the clinical information provided by FoCUS. In color doppler, red indicates the flow of blood toward the probe, while blue indicates flow away from the probe. An example of this application is when color-flow doppler is applied to the mitral valve in the A4C views. A blue-colored jet of flow going from the left ventricle to the left atrium during ventricular systole indicates mitral valve regurgitation. A useful application of PW doppler is to quickly estimate cardiac output. This is done by obtaining the A5C view by first obtaining the A4C view and tilting the probe slightly cephalad, until the aortic valve (AV) and left ventricular outflow tract (LVOT) appear. The PW doppler is then applied, and the doppler gate (two horizontal lines) positioned approximately 1 cm above the AV within the LVOT, before activating the PW doppler. Tracing the systolic waveform begets the LVOT velocity time integral (VTI). An LVOT VTI of less than 18 cm suggests low cardiac output.
Competency in FoCUS image acquisition requires appropriate training and quality assurance. Clinicians should complete a minimum portfolio under the supervision of a mentor. as recommended by various societal bodies13,14. The stereotactic and psychomotor aspects of FoCUS require repetition, time, and experience to achieve mastery. The experience should include the performance of exams on patients with varying body habitus in a diversity of clinical settings.
There are some clinical scenarios in which limitations cannot be overcome. A skilled provider recognizes situations in which FoCUS should not be performed and pursues alternative investigations, such as transesophageal echocardiography or formal comprehensive transthoracic echocardiogram. Adequate images cannot be obtained in patients who have an open chest or have diffuse subcutaneous emphysema affecting the chest wall. Indiscriminate use of FoCUS may lead to further unnecessary testing, unnecessary interventions resulting from false positive findings, or inadequate workup of false negative findings2. FoCUS should not be used for the identification of subtle abnormalities. Although transducers that are used for FoCUS have become more compact and portable, these devices do not possess the complex image enhancement, artifact reduction abilities, and higher resolution capabilities of state-of-the-art instruments used in formal echocardiography15. Diagnosis of complex and unusual cardiac pathologies is outside the scope of FoCUS. Quantification of regurgitant or stenotic valvular lesion severity should not be performed using FoCUS alone. Instead, FoCUS should be used to detect significant deviations from normal, and are usually reported as "present" or "absent"15.
Although FoCUS has been well established within the cardiology community for decades, its use is now virtually ubiquitous in emergency medicine and critical care, and is expanding into other care settings16. As ultrasound technology improves, and devices become more portable, FoCUS is becoming an important tool for both diagnosis and guiding management of cardiac disease. Over time, competency in FoCUS can be achieved through a structured and consistent approach to exam sequence, use of appropriate terminology, and the development of stereotactic and psychomotor skills.
FoCUS is a limited, problem oriented application of echocardiography which is rapidly expanding in the clinical environment. Competency in FoCUS includes mastery of the stereotactic and psychomotor skills required for transducer manipulation and image acquisition. Competency also requires the ability to optimize the setup, troubleshoot image acquisition, and understand the sonographic limitations due to complex clinical environments and patient pathology. We describe methods of transducer manipulation, review common pitfalls of transducer movements, and suggest tips to optimize phased array transducer use.
Disclosures
The authors have nothing to disclose.
Acknowledgements
We would like to thank the University of Michigan Department of Anesthesia, Max Harry Weil Institute for Critical Care Research and Innovation, and Katelyn Murphy for their administrative and graphic design support.
Materials
| Aquasonic ultrasound gel | Parker | 30592052 | https://dr.graphiccontrols.com/en/catalog/ultrasound-gel/parker-laboratories-01-50-aquasonic-100-gel-5l-1332e66e/ |
| Philips Sparq ultrasound machine | Phillips | https://www.usa.philips.com/healthcare/product/HC795090CC/sparq-ultrasound-system#documents |
References
- Birch, M. S., Marin, J. R., Liu, R. B., Hall, J., Hall, M. K. Trends in diagnostic point-of-care ultrasonography reimbursement for medicare beneficiaries among the US emergency medicine workforce, 2012 to 2016. Annals of Emergency Medicine. 76 (5), 609-614 (2020).
- Moore, C. L., Copel, J. A. Point-of-care ultrasonography. The New England Journal of Medicine. 364 (8), 749-757 (2011).
- Su, E., Dalesio, N., Pustavoitau, A. Point-of-care ultrasound in pediatric anesthesiology and critical care medicine. Canadian Journal of Anaesthesiology. 65 (4), 485-498 (2008).
- Niblock, F., Byun, H., Jabbarpour, Y. Point-of-care ultrasound use by primary care physicians. The Journal of the American Board of Family Medicine. 34 (4), 859-860 (2021).
- Coritsidis, G. N., et al. Point-of-care ultrasound for assessing arteriovenous fistula maturity in outpatient hemodialysis. The Journal of Vascular Access. 21 (6), 923-930 (2020).
- Gundersen, G. H., et al. Adding point of care ultrasound to assess volume status in heart failure patients in a nurse-led outpatient clinic. A randomised study. Heart. 102 (1), 29-34 (2016).
- Kirkpatrick, J. N., et al. Recommendations for echocardiography laboratories participating in cardiac point of care cardiac ultrasound (POCUS) and critical care echocardiography training: report from the American Society of Echocardiography. Journal of the American Society of Echocardiography. 33 (4), 409-422 (2020).
- Annals of Emergency Medicine. Ultrasound Guidelines: Emergency, point-of-care and clinical ultrasound guidelines in medicine. Annals of Emergency Medicine. 69 (5), 27-54 (2017).
- Levitov, A., et al. Guidelines for the appropriate use of bedside general and cardiac ultrasonography in the evaluation of critically ill patients-part II: cardiac ultrasonography. Critical Care Medicine. 44 (6), 1206-1227 (2016).
- Neskovic, A. N., et al. Focus cardiac ultrasound core curriculum and core syllabus of the European Association of Cardiovascular Imaging. European Heart Journal. Cardiovascular Imaging. 19 (5), 475-481 (2018).
- Mitchell, C., et al. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. Journal of the American Society of Echocardiography. 32 (1), 1-64 (2019).
- Dinh, V. A., et al. Measuring cardiac index with a focused cardiac ultrasound examination in the ED. The American Journal of Emergency Medicine. 30 (9), 1845-1851 (2012).
- Expert Round Table on Echocardiography in ICU. International consensus statement on training standards for advanced critical care echocardiography. Intensive Care Medicine. 40 (5), 654-666 (2014).
- Expert Round Table on Echocardiography in ICU. International expert statement on training standards for critical care ultrasonography. Intensive Care Medicine. 37 (7), 1077-1083 (2011).
- Spencer, K. T., et al. Focused cardiac ultrasound: recommendations from the American Society of Echocardiography. Journal of the American Society of Echocardiography. 26 (6), 567-581 (2013).
- Nelson, B. P., Sanghvi, A. Point-of-care cardiac ultrasound: feasibility of performance by noncardiologists. Global Heart. 8 (4), 293-297 (2013).
