1. Mouse Bladder Wall Injection
Choice of mouse strain, age, and sex is dictated by experimental needs. We use mice between 8 and 12 weeks of age, since this is a window of immunological maturity prior to senescence. As a general guideline, mice should arrive at least one week prior to experimental manipulation in order to avoid stress-induced confounding factors.
- Clean the surgical table surface with soap and water.
- Wipe the surgical table surface with Cide Swipes or antiseptic wipes.
- Autoclave clean surgical instruments prior to use in surgery.
- In addition, sterilize surgical instruments with hot bead sterilizer immediately prior to use, as well as between animals during surgery.
- Clean 100 μL Hamilton syringes and 29 or 30 gauge (1/2 inch long) needles by repeated aspiration and injection with absolute alcohol before first use and at the end of the final surgical procedure.
- Wash and rinse Hamilton syringes with sterilized phosphate-buffered saline between each animal.
- Anesthetize mice by placing them in an isoflurane induction chamber, with the isoflurane set between 2-5%.
- Once general anesthesia is achieved, remove the mouse from the chamber and place in the supine position with a warm pad underneath to help maintain normal body temperature.
- Achieve maintenance anesthesia by placing the animal’s snout in a nozzle containing vaporize isoflurane (titrated from 1-3% as necessary to maintain appropriate anesthesia).
- Shave the abdominal skin with clippers.
- Use a disposable, sterile surgical drape to cover the anus to prevent fecal contamination during surgery.
- Use a second disposable, sterile surgical drape to cover the surgical field (lower abdomen).
- Prep the abdomen with three pieces of Betadine-soaked gauze. Repeat this step three times.
- Using a dissecting microscope for magnification, make a lower midline abdominal incision with scissors.
- Expose the bladder.
- If the bladder is full, partially decompress it by gentle downward pressure at the dome.
- Inject the sample solution (up to 50 μL), using a 29 or 30 gauge needle and syringe, into the wall of the bladder dome (intramural injection) with the bevel of the needle facing upwards.
- Push the plunger of the syringe to inject the sample solution into the bladder wall. A well-localized bleb is an indication of successful injection of the cells into the bladder wall.
- Remove the syringe, close the incision with wound clips and allow the mouse to recover on a warming pad.
2. Representative Results:
A well-localized bleb that does not leak fluid and stays stable in size is an indication of successful injection of the cells into the bladder wall (Figure 1). Histological analysis can be performed to confirm the presence of the injected cells in the bladder wall.

Figure 1. Example of successful bladder wall injection using India ink for illustration.
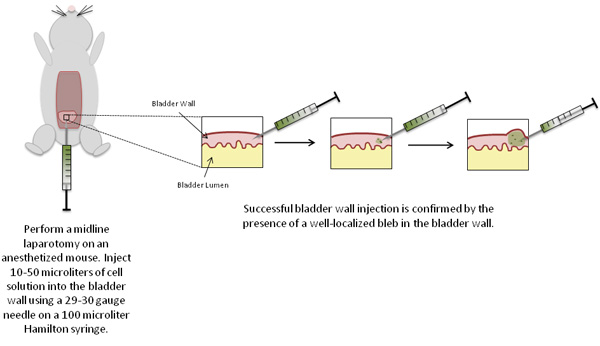
Figure 2. Schematic of experimental procedures.
