The basic principles and workflow of the 3-plex assay are shown in Figure 1, and the overall workflow is described in Table 1. Uniplex assays work along the same principle except that the entire bottom well is coated with one capture antibody. Signal detection is done by ECL in which an electrical signal is applied to the bottom of the well. This, in turn, initiates a local production of light through a chemical reaction of the read-buffer with the SULFO-TAG label on the detection antibody. This leads to the low background and high sensitivity of the assay. In Figure 2, the standard curve of cMyBP-C in the uniplex assay is compared to that of cMyBP-C in the 3-plex assay. Both assays show a very high sensitivity and a high dynamic range. Detection levels and quantification levels are shown in Table 2 and are comparable in both uniplex and 3-plex assays. Detection levels for cTnI and CK-MB are also shown in Figure 3 and Table 2. Inter-operator variability was determined by measuring identical samples (n = 2, 3 technical replicates) by two different operators and variability was found to be low (CV 8.5%). Cross reactivity of detection antibodies with the other two calibrators was studied by incubating individual standard curves of all three calibrators with single detection antibodies (Figure 4). Only low amount of cross-reactivity was seen between CK-MB calibrator and both cTnI and cMyBP-C detection antibodies while no cross-reactivity was observed between the other calibrators and detection antibodies.
As proof of the applicability of the assay for the detection of cardiac injury, serum levels of 16 subjects with MI were compared with a control group (n = 16). Using the 3-plex plate, serum levels of cMyBP-C, CK-MB, and cTnI were determined. All three biomarkers were increased in the MI subjects (see Figure 5) from 3.7-fold (cMyBP-C) to 12.2-fold (CK-MB), although variation in serum levels was the lowest in the cMyBP-C group.
| Process | Uniplex assay | 3-plex assay | |
| Experiment day 0 | Coat plate with capture antibody | Overnight | N/A |
| Experiment day 1 | Block the plate | 1 hr | 30 min |
| Prepare samples and standard series | |||
| Incubate with samples and standards | 1 hr | 2 hr | |
| Incubate with detection antibody | 1 hr | 1 hr | |
| Add detection reagent and read plate |
Table 1. Workflow overview of uniplex and multiplex assays.
| LLOD (ng/ml) | LLOQ (ng/ml) | ULOQ (ng/ml) | |
| cMyBP-C (uniplex) | 0.126 ± 0.007 | 0.567 ± 0.073 | 400 ng/ml |
| cMyBP-C (3plex) | 0.057 ± 0.022 | 0.469 ± 0.171 | 400 ng/ml |
| CK-MB (3-plex) | 0.038 ± 0.014 | 0.587 ± 0.213 | 100 ng/ml |
| cTnI (3plex) | 0.033 ± 0.011 | 0.147 ± 0.053 | 25 ng/ml |
Table 2. Detection limits of uniplex and 3-plex calibrators. LLOD, lower limit of detection, is defined as calculated concentration of the signal of the blank + 3 times standard deviation of the blank samples. LLOQ, lower limit of quantification, is defined as a value higher than LLOD, with a coefficient of variance (reciprocal of signal to noise ratio) lower than 20%, and a recovery between 80 – 120%. ULOQ, upper limit of quantification, is defined as the highest analyzed concentration that can be measured with a coefficient of variance lower than 20% and a recovery between 80 – 120%.
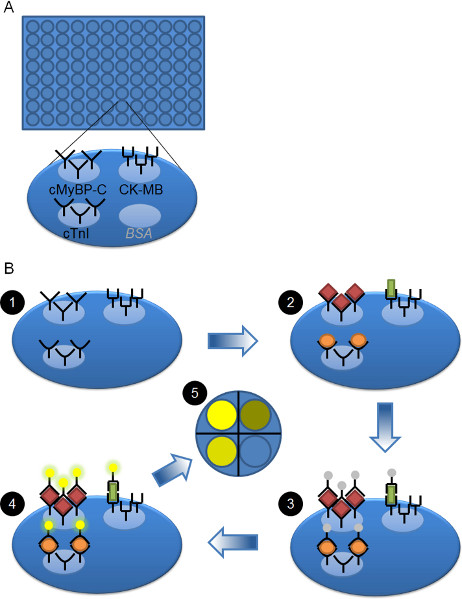
Figure 1. Schematic overview of plate and workflow. A) 96 well plate is shown. Each well is coated with three different capture antibodies, i.e. against cMyBP-C, CK-MB and cTnI. The fourth available spot is not used and is coated with BSA. B) Workflow of the 3-plex ELISA. The pre-coated plate (step 1) is blocked and then serum samples or calibrators are added to each well and allowed to bind (step 2). cMyBP-C (red diamonds), CK-MB (green rectangle), and cTnI (orange oval) bind to their respective capture antibodies. After washing away the unbound proteins, the SULFO-TAG-labeled detection antibodies are added (step 3). They will bind to the cMyBP-C, CK-MB, or cTnI proteins that are bound to their capture antibody. After washing away unbound detection antibody, read buffer is added and the plate is analyzed. An electrical signal to the bottom of the plate initiates a local chemical reaction of the SULFO-TAG with the read buffer, leading to the production of light (step 4). The amount of light is directly proportional to the amount of SULFO-TAG labeled detection antibody bound. The CCD imager records the light and can distinguish the different spots within each well and therefore the signal coming from each analyte (step 5).
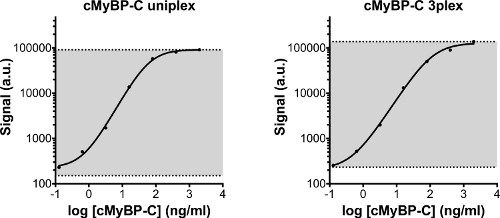
Figure 2. Standard curve of cMyBP-C calibrator measured in uniplex or in 3-plex. The same standard series was measured in a uniplex assay, and on the 3-plex plate. The standard series started at 2,000 ng/ml and was serially diluted 5x with the lowest concentration being 0.128 ng/ml. In addition, diluent was used as a blank sample. The detection area of the assay is displayed in grey. The lower line indicates the lower limit of detection (LLOD), which is defined as the calculated concentration of the blank signal + 3 times the standard deviation of the blank values. The upper limit of detection is defined as the highest concentration of the standard series that can reliably be measured. Both uniplex and 3-plex cMyBP-C standard curves are comparable. Detection limits are displayed in Table 2. a.u: arbitrary units.
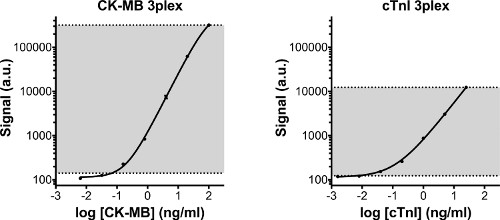
Figure 3. Standard curves of CK-MB and cTnI. Standard curves of CK-MB and cTnI, which were measured simultaneously with cMyBP-C on the 3-plex plate. Both calibrators show high sensitivity and a large dynamic range. In gray the detection area of the assay is displayed. The lower line indicates the lower limit of detection (LLOD), which is defined as the calculated concentration of the blank signal + 3 times the standard deviation of the blank values. The upper limit of detection is defined as the highest concentration of the standard series that can reliably be measured. Detection limits are displayed in Table 2. a.u: arbitrary units.
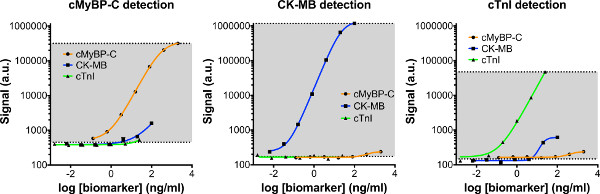
Figure 4. Cross-reactivity of 3-plex detection antibodies. Separate standard curves of cMyBP-C, CK-MB, and cTnI were prepared and incubated on the 3-plex plate. Each standard curve was than probed with individual detection antibodies, to assess the amount of cross-reactivity between individual detection antibodies (e.g. cMyBP-C) and the other calibrators (e.g. CK-MB and cTnI). Cross-reactivity was low in the 3-plex assay. Click here to view larger figure.
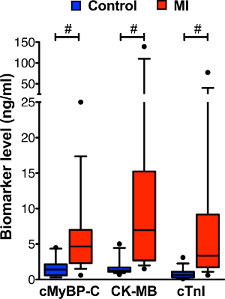
Figure 5. Biomarker levels in serum of MI and control subjects measured with 3-plex assay. Levels of cMyBP-C, CK-MB, and cTnI were measured simultaneously by 3-plex assay in serum samples of 16 control subjects and 16 subjects with MI. Data is displayed by box and whisker plots (whiskers represent 10th and 90th percentile). Increased levels of all three biomarkers were observed in the serum of subjects with MI compared with the control group. Because the data did not show a normal distribution (tested by D’Agostino Pearson Omnibus), the non-parametric Mann-Whitney statistical test was used to test for differences between control and MI groups. # P < 0.001
