Figure 5 depicts the range in measured and calculated values obtained by performing morphometric analysis on wild-type wounds generated in different mouse strains by multiple surgeons and analyzed by different individuals. Wild-type mice from different strains can display statistical differences as described both in our studies and in the literature9,10. Based on these representative results, we recommend that, within one study, mice from only one strain be used. Although we recommend that the same individual perform all the wounds within a particular study, multiple individuals could act as surgeons as long as the area of the wounds at day 0 is not statistically different between individual’s work. Finally, because the morphometric analysis described in this protocol can be extensive, multiple individuals could analyze parts of the same experiment, but only if the results of their analysis of two samples are within 5% of each other. However, it is preferable to have a single individual analyzing the wounds in a blinded manner to avoid bias.
Figure 6 displays a meta-analysis comparing wound measurements obtained by following the protocol described in this study11 with measurements obtained from the “middle” of the wound and 40 surrounding sections. In Figure 6A, the epidermal area and wound area were calculated from the measurement of the epidermal and wound lengths on wound sections followed by the calculation of the percentage of the epidermal area among wound area (sometimes referred to as “percentage of closure” or “percentage of epithelialization”). Similarly, in Figure 6B, the percentage of the epidermis in the wound was obtained as the ratio of the epidermal volume (calculated from the measured epidermal area) over the wound volume (calculated from the measured wound area). For both parameters, the analysis of the whole wound showed strong statistical differences between groups (up to P < 0.001 following One-way Anova). However, the significance was decreased (up to P < 0.01 following One-way Anova) when only 40 sections in the middle of the would were analyzed. These results demonstrate a decrease in the level of significance when only a subset of the wound is analyzed. These data suggest that defects with a small effect size will likely only be detected when performing morphometric analysis on the entire wound, and that more mild wound healing phenotypes will be missed from a “middle of the wound” type of analysis.
Common practice for analyzing in vivo wound healing involves measuring the area of the wound on histological sections chosen somewhere in the wound12. With that in mind, the average of the measured wound area from the serial sections of entire wounds was compared with the one obtained from the middle subset sections. The results showed no significant difference between experimental groups and between method of analysis (Figure 6C). However, the current protocol uses the measured area (shown in Figure 6C) over the whole wound to calculate the wound volume. As shown in Figure 6D, the calculated wound volume (which can only be calculated using the analysis of the whole wound) is significantly different between the experimental groups. In sum, these representative results demonstrate the importance of in-depth histological analysis of wound healing parameters described in this protocol in order to detect phenotypes that would otherwise have been missed using a more traditional wound healing analysis.
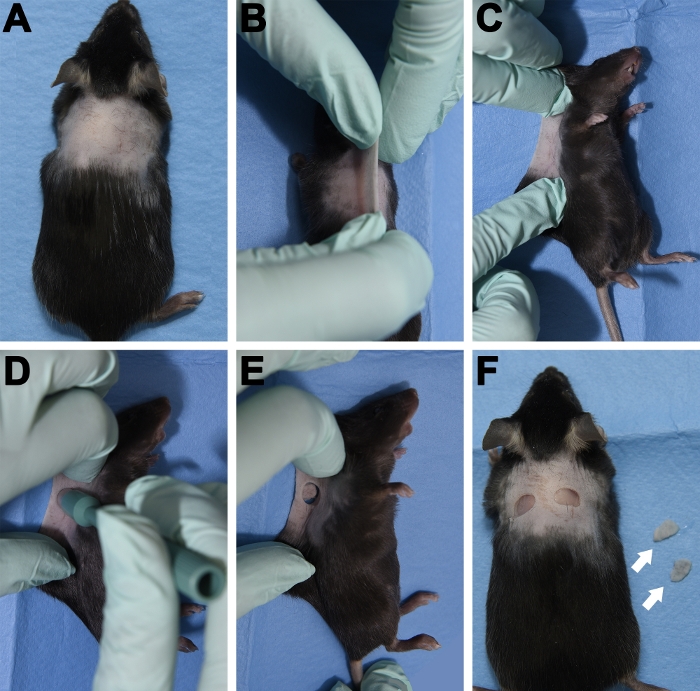
Figure 1: Bilateral excisional wound procedure. (A) Representative photograph of a mouse after clipping and shaving hair from the surgical area. (B) The skin pinched between the shoulder blades along the dorsal midline. (C) The mouse positioned on its side with the skinfold laid flat. (D) Representation of the biopsy punch placement. (E) Punched skinfold. (F) The mouse with two bilateral wounds at day 0 and the excised punch biopsy control tissues as indicated by the white arrows. Please click here to view a larger version of this figure.
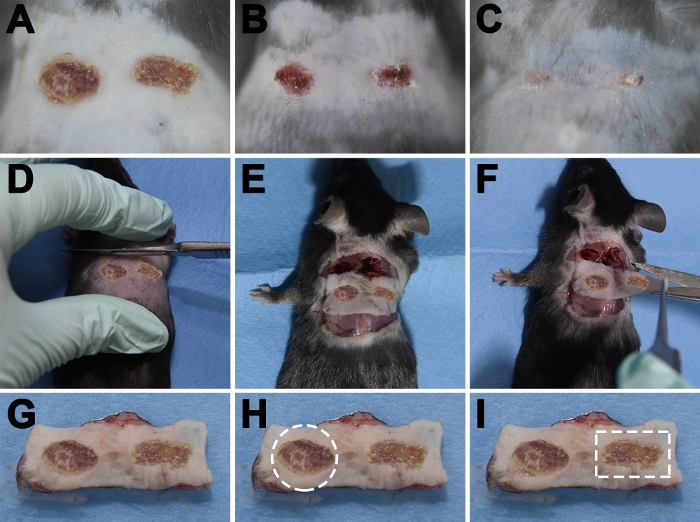
Figure 2: Wound harvest procedure. (A-C) Macroscopic photographs of 6 mm excisional wounds after 4 days (A), 7 days (B) and 11 days (C). (D-E) With a scalpel blade, a cutaneous incision was made in the shape of a wide rectangle that includes the wounds and surrounding unwounded tissue. (F) The skin was released from underlying tissue with forceps and scissors. (G) Representation of harvested bilateral wounds. (H) The dotted white line represents the border of the tissue that would be harvested following the use of a punch biopsy (this method allows for standardized amount of tissue harvested). (I) The dotted white line represents the border of the tissue that would be trimmed for histology (rectangular shape allows for easier embedding). Please click here to view a larger version of this figure.
| Solution | Time (minutes) | Temperature (Celsius) | Pressure (kPa) |
| 80% ETOH | 30 | RT | N/A |
| 95% ETOH | 30 | RT | N/A |
| 100% ETOH | 30 | RT | N/A |
| Xylene | 30 | RT | N/A |
| Xylene | 30 | RT | N/A |
| Paraffin | 30 | 60 | 20 |
| Paraffin | 30 | 60 | 20 |
Table 1: Sample processing procedure for paraffin embedding. RT = room temperature. N/A = not applicable.
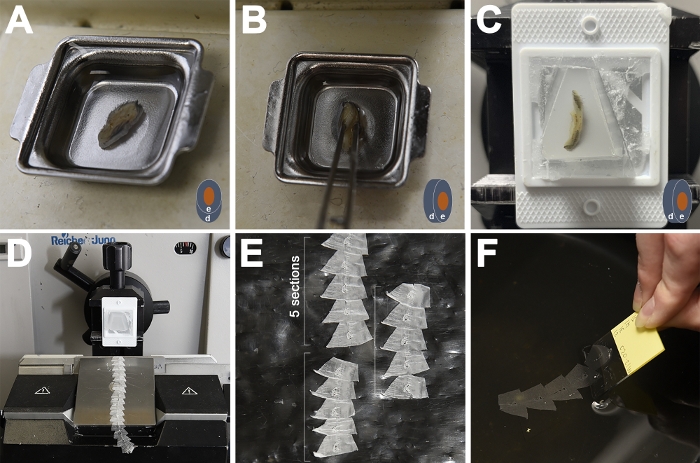
Figure 3: Wound embedding and sectioning. (A) Paraffin-processed wound lying flat in an embedding mold. (B) The wound was held at 90˚ (“standing”) from the horizontal surface of the mold for embedding. (C) Paraffin-embedded wound properly oriented for sectioning (D) Paraffin block mounted on the microtome was sectioned into ribbons of about 20 sections (E) Paraffin ribbons cut in 5-section increments as indicated by the white brackets. (F) Serial sections laid flat in a warm water bath (40-45 ˚C) were mounted on a microscope slide. The cartoon in (A-C) represents the wound (orange) in the skin (blue) with the proper orientation of the epidermis (e) and the dermis (d) for each step. Please click here to view a larger version of this figure.
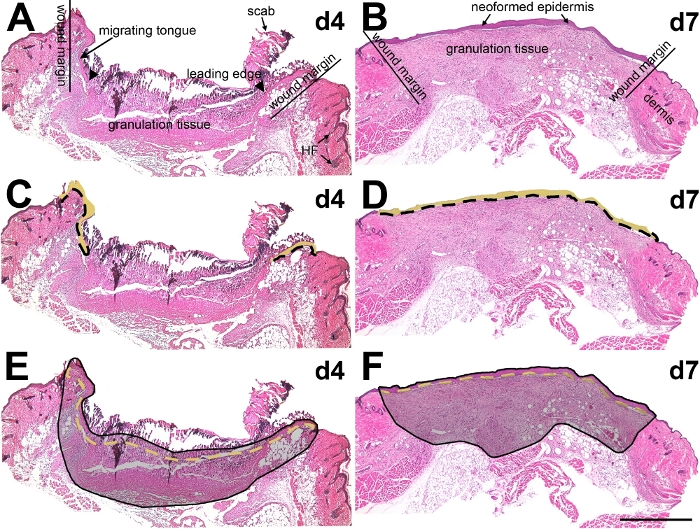
Figure 4: Histological characteristics of wounds and illustration of morphometric parameters. (A, B) Histological features of a day 4 (A) and a day 7 (B) 6 mm wound. (C-F) Representation of the different measurements used to perform the quantitative morphometric analysis: length of the epidermis (C, D, dotted black line), measured area of the epidermis (C, D, yellow shaded area), length of the wound (E, F, dotted yellow line) and measured area of the entire wound (E, F, gray shaded area). HF = hair follicle; scale bar = 1 mm. Please click here to view a larger version of this figure.
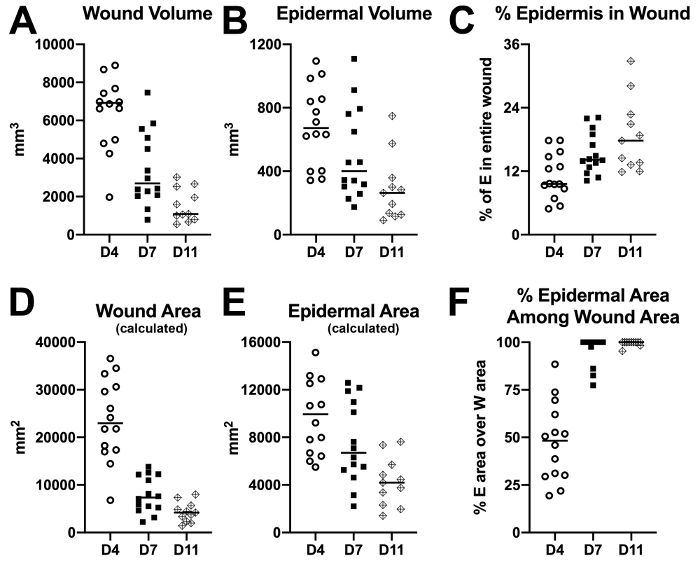
Figure 5: Morphometric characteristics of representative 6 mm wild-type wounds at day 4, day 7 and day 11 post-wounding. Scattered plots represent data obtained from morphometric analyses of 6 mm wild-type wounds generated in different mouse strains by multiple surgeons and analyzed by different individuals. (A) wound volume, (B) epidermal volume, (C) percentage of epidermis in the wound, (D) wound area (calculated), (E) epidermal area (calculated), and (F) percentage of epidermal area among wound area demonstrate the range of variation in morphometric values. Please click here to view a larger version of this figure.
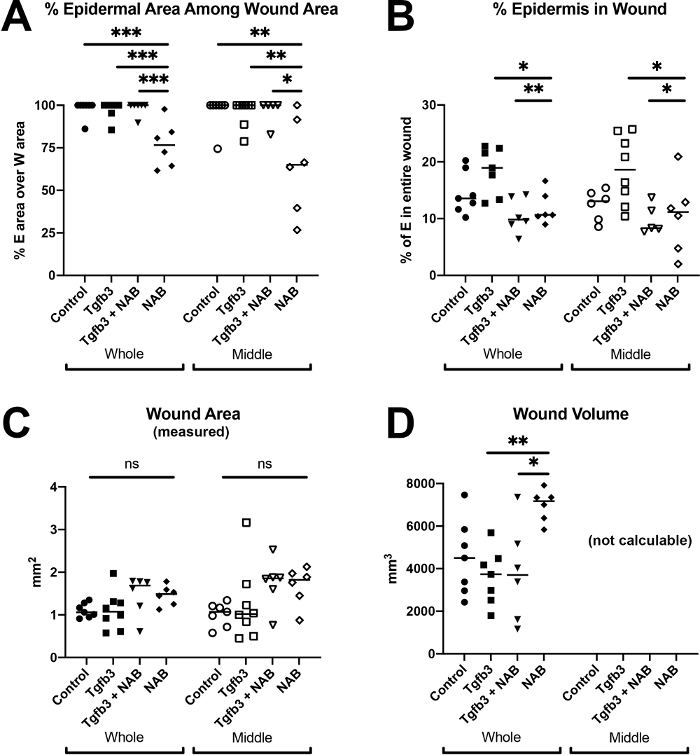
Figure 6: Meta-analysis comparing parameters obtained from whole wound with middle of the wound identifies new defects with higher significance. Wound healing morphometry was performed on day 7 wounds injected with saline (control), transforming growth factor beta 3 (Tgfb3), Tgfb3 with neutralizing antibody (Tgfb3 + NAB) and neutralizing antibody alone (NAB). Measurements were performed on serial sectioned wounds (“whole”) or on 40 sections from the middle of the wound (“middle”) and used to calculate the percentage of epidermal area over wound area (A), the percentage of epidermis in the wound (B), and the wound volume (D). (C) represents the average of the wound area measured on the whole or middle of the wound. * P < 0.05, ** P < 0.01, *** P < 0.001, ns = not significant, One-way Anova). This figure has been modified using data from Le et al.11. Please click here to view a larger version of this figure.
Supplementary Table 1: An example of a spreadsheet for recording morphometric measurements. Please click here to download this table.
