On postoperative day #1, the patient presented in the video underwent a CT of the head and an x-ray of the abdomen (Figure 7). This imaging, respectively, demonstrated optimal proximal catheter placement in the right lateral ventricle and the location of the distal catheter in the peri-hepatic space. At the patient's 3-month and 1-year postoperative clinic assessments following placement of the VP shunt, his gait velocity had improved from a preoperative 0.83 m/s to 1.4 m/s and his MoCA score had normalized at 29/30 from a preoperative score of 22/30.
The feasibility and patient outcomes of the surgical approach presented here were examined in a 7-year prospective continuous quality improvement study, which has now been reported in reference36. In summary, 224 consecutive adult patients were enrolled at a tertiary center36. The primary objective was to determine the combined role of neuronavigation and laparoscopy with a shunt infection prevention strategy to reduce the incidence of VP shunt insertion failure. Of those patients, 115 underwent VP shunt insertion without neuronavigation and/or laparoscopy guidance (Pre-ShOut), and 129 patients (Post-ShOut) were treated with the surgical approach presented here (Table 1). We found that a background of shunt infection reduction protocols and combined neuronavigation and laparoscopy were associated with a reduction in overall shunt failure rates from 37% to 14%, 45% to 22% and 51% to 29% at 1 year, 2 year and 3 year, respectively (Hazard Ratio 0.44; p<0.001) (Figure 8). There were no proximal catheter failures when neuronavigation was used. The 2 year rates of distal catheter failure were 42% versus 20% among the patients who did not versus those who did undergo the combined neuronavigation and laparoscopy-guided VP shunt surgery, respectively (p<0.001).
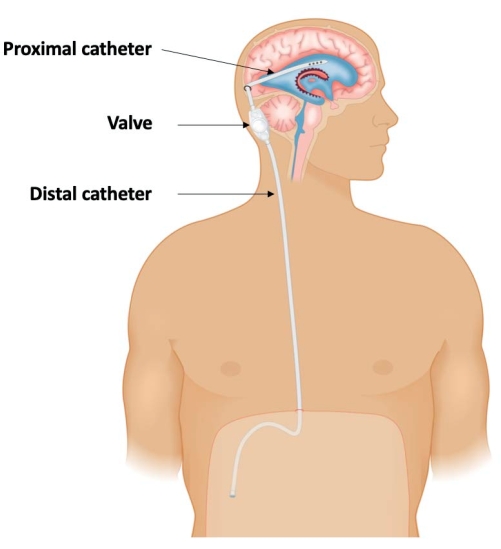
Figure 1: Schematic demonstrating the three-component configuration of a ventriculoperitoneal shunt: A proximal catheter placed within the lateral ventricle; connected to a valve that regulates cerebrospinal fluid (CSF) drainage; and a distal catheter that diverts the CSF into the peritoneal cavity to be absorbed. This figure has been adapted from Isaacs et al.36. Please click here to view a larger version of this figure.
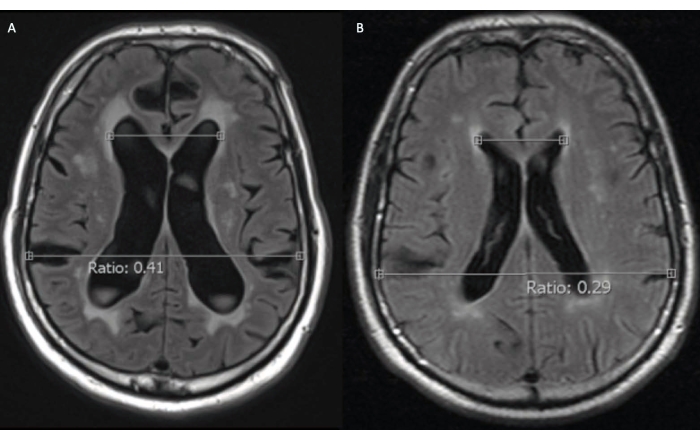
Figure 2: Axial T2 fluid-attenuated inversion recovery magnetic resonance imaging (MRI) of a 72-year-old male idiopathic normal pressure hydrocephalus patient before surgical treatment. (A) At presentation, the patient had hydrocephalus (Evans ratio 0.41). (B) An MRI scan obtained 4 years prior to presentation, for an unrelated indication, did not have any evidence of pathological ventricular dilatation (Evans ratio 0.29). Please click here to view a larger version of this figure.
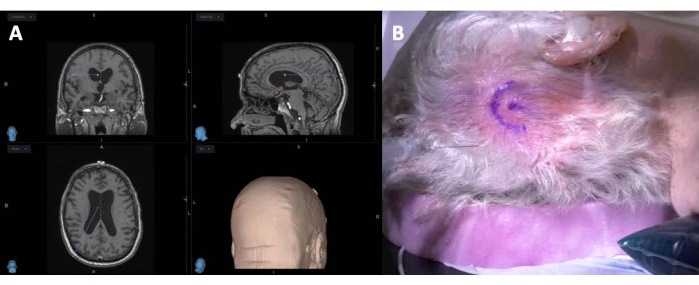
Figure 3: Preoperative planning of a ventriculoperitoneal shunt insertion. Left (A) is a screen-capture of a neuronavigation station for planning the trajectory and entry point for the proximal VP shunt catheter. Right (B) shows a horseshoe-shaped incision marked in the right occipital region to incorporate the catheter entry point. Please click here to view a larger version of this figure.
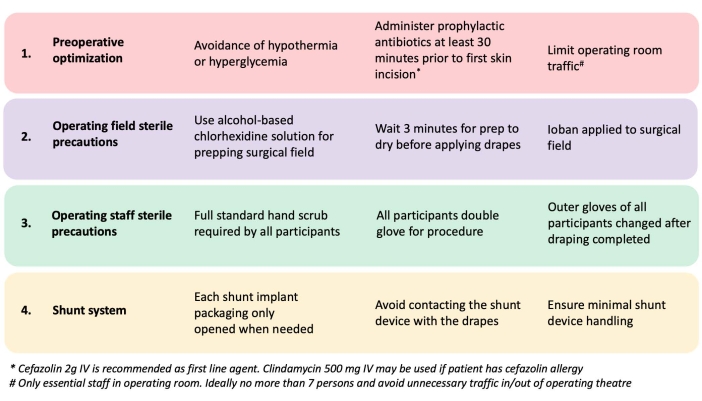
Figure 4: A shunt infection prevention strategy. This is adapted from Muram et al.38. Please click here to view a larger version of this figure.
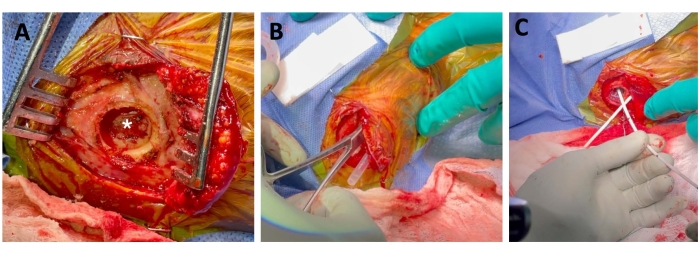
Figure 5: Proximal ventriculoperitoneal shunt catheter insertion under neuronavigation guidance. Left (A) shows the reflected scalp and a burr hole with preservation of the dura (star). Middle (B) depicts the tunneled sheath from the sub-xiphisternum to the cranial incision, and creation of the subgaleal pocket for the shunt valve. Right (C) demonstrates the inserted proximal catheter. Please click here to view a larger version of this figure.
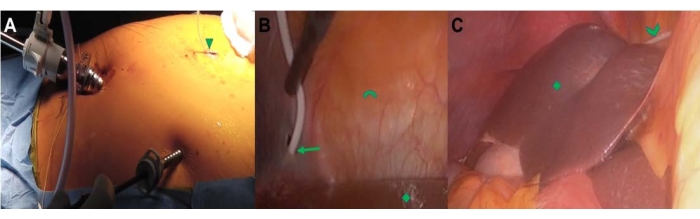
Figure 6: Laparoscopic-guided insertion of distal VP shunt catheter. Left (A) demonstrates the general abdominal setup of a three-port system, with the distal catheter through a sub-xiphisternum incision (triangle). Middle (B) demonstrates the traversing distal catheter guided through a hole created in the falciform ligament (arrow). The liver (diamond) and abdominal wall (arc) are shown. Right (C) depicts the final placement of the distal catheter (chevron) over the dome of the liver (diamond) with the catheter tip located in the pericolic gutter. Please click here to view a larger version of this figure.
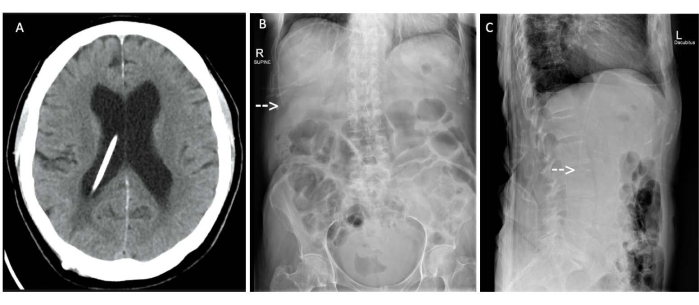
Figure 7: Tomography and X-rays. (A) Axial computed tomography head scan and (B) anteroposterior and (C) lateral abdominal X-rays of a 72-year-old male idiopathic normal pressure hydrocephalus patient following placement of a ventriculoperitoneal shunt. (A) The proximal catheter placed under neuronavigation is optimally placed within the right lateral ventricle and (B, C, arrows) the distal catheter placed laparoscopically is optimally located in the right upper quadrant within the peri-hepatic space. Please click here to view a larger version of this figure.
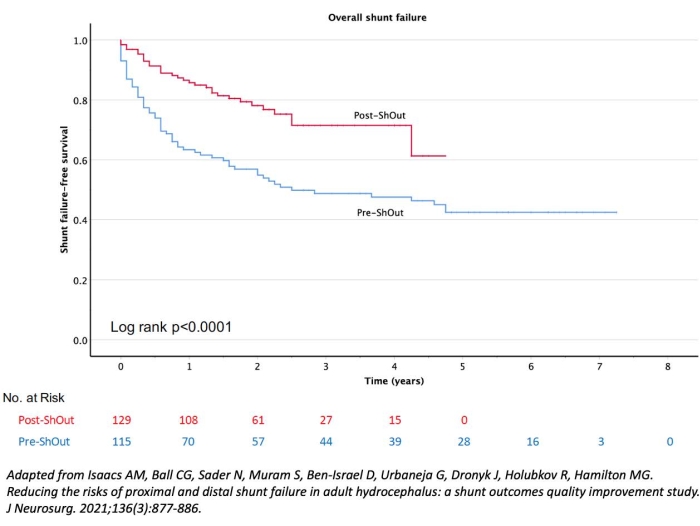
Figure 8: Kaplan Meier analysis of overall shunt-failure free survival in 224 patients who underwent ventriculoperitoneal (VP) shunt insertion. The rates of overall shunt failures were significantly higher in the 115 patients who underwent VP shunt insertion without neuronavigation and/or laparoscopy guidance (Pre-ShOut), than the 129 patients who had their VP shunts placed with neuronavigation and laparoscopy guidance (Post-ShOut). This figure has been adapted from Isaacs et al.36 Please click here to view a larger version of this figure.
Table 1: Baseline demographics and outcomes of patients who underwent ventriculoperitoneal shunt with (Post-ShOut) or without (Pre-ShOut) neuronavigation and/or laparoscopy. This table has been adapted from Isaacs et al.36 Please click here to download this Table.
