After practice, survival on the first post-operative day is typically over 95%; at post-operative day 7, survival was 91.3%. Figures 1 and 2 show the ideal puncture site in coronal and cross-sectional views; placement of the puncture site is critical to obtaining good survival without excessive hemorrhage. Intra-operative deaths and early post-operative deaths are typically due to hemorrhage. This tends to occur with excessive dissection between the aorta and the IVC, or from inadequate hemostatic pressure. Figure 3 shows a schematic of the importance of wrapping the puncture site with connective tissue prior to applying pressure for hemostasis, allowing good hemostasis without compression of the AVF. In our experience, all technically successful AVF can be confirmed with ultrasound by the third day; once the AVF is confirmed on duplex to be present, the AVF will usually be stable at least until day 28. Figure 4 shows typical Doppler ultrasound findings in successful AVF formation. Changes in waveforms were observed at the level of the AVF in IVC and towards the heart. The overall AVF confirmation rate on post-operative day 3 was 71.4%.
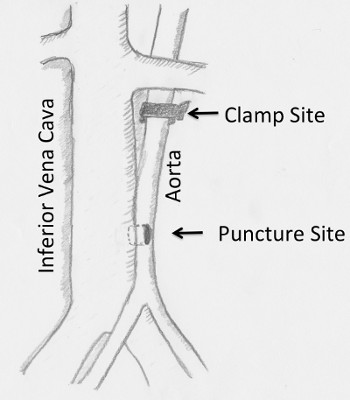
Figure 1. Diagram showing the puncture site. The ideal puncture site is between half to three quarters of the distance between the left renal vein and iliac bifurcation. IVC: Inferior vena cava.
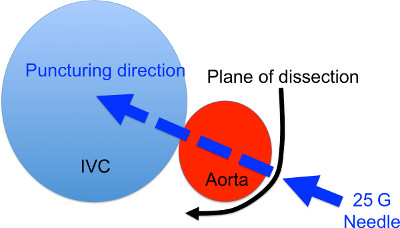
Figure 2. Cross section diagram of the AVF formation site. The black arrow denotes the site and direction of dissection to expose the aorta. The blue arrow denotes the puncturing site and direction.
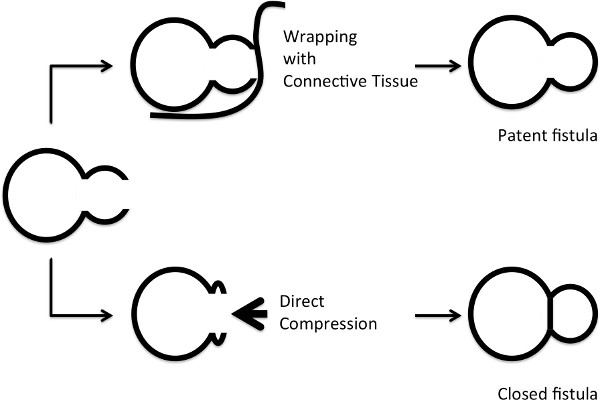
Figure 3. Diagram showing the method for hemostasis. Upper row: wrapping the aorta with connective tissues and muscles. Lower row: applying direct pressure. The chances of AVF closure are high with direct compression.
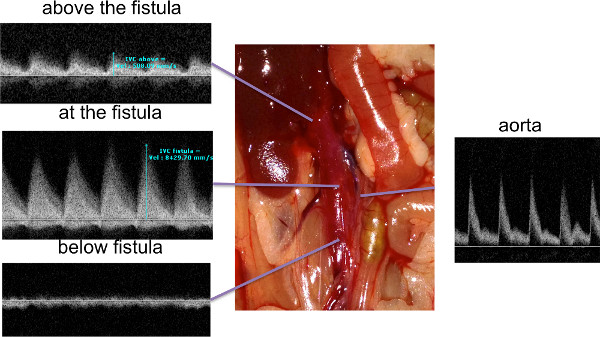
Figure 4. Ultrasound findings after AVF surgery. The AVF was examined with high-resolution ultrasound post-operatively. Waveforms below the AVF were typical venous waveforms, whereas at and above the AVF the waveforms showed superimposition of arterial flow that was not present below the AVF. Click here to view larger figure.
