Male mice underwent the operation mentioned above to create both an AVF and an IVC stenosis. Control mice underwent only laparotomy and dissection of the tissues surrounding the IVC, e.g., a sham procedure, or only creation of an IVC stenosis without simultaneous creation of an AVF.
The IVC was observed with Doppler ultrasound on day 7 after the surgical procedure (Figure 2). The fistula and stenosis areas of the IVC were easily detected in the longitudinal view (Figure 2C,E). The IVC between the fistula and the stenosis was dilated in mice having an AVF with the stenosis. The ultrasound waveforms were examined in the IVC at the point of the stenosis (Figure 2D,F). In mice bearing a stenosis alone, without an AVF, the stenosis segment showed a venous waveform with more spectral broadening than sham-operated mice but without much pulsatility. However, in mice having an AVF as well as a stenosis, the stenosis segment showed a pulsatile waveform in addition to spectral broadening. The time-averaged maximum velocity of the flow at the stenosis in mice having an AVF with stenosis was significantly higher than mice having stenosis alone (Table 1).
The Doppler ultrasound B mode was used in transverse views to assess the IVC on day seven after surgery (Table 1). The mean IVC diameter at the stenosis in mice having stenosis alone was similar to the mice having an AVF as well as the stenosis (Table 1). The percent stenosis of the IVC was calculated according to the NASCET method12. Using either the upstream segment or the downstream segment as the reference, the percent stenosis was significantly greater in mice having an AVF in addition to the stenosis (Table 1).
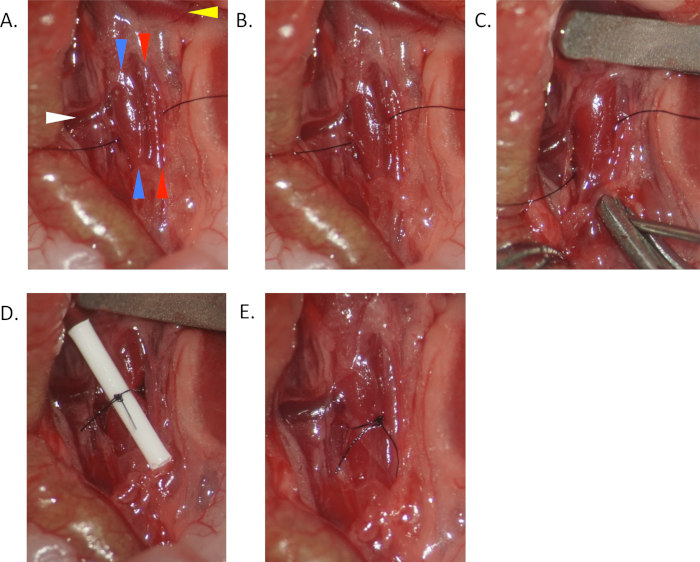
Figure 1. Operative photos of murine AVF model with venous stenosis. (A) Place an 8-0 suture beneath the IVC (blue arrowheads) and aorta (red arrowheads) halfway between the left renal vein (yellow arrowheads) and the aortic bifurcation, distally to any large IVC branches if present. (B) Place the suture beneath the IVC only. (C) After proximal clamping, puncture the aorta through both walls and into the IVC. (D) Tie a tip of a 22 G IV catheter and the IVC together with the placed suture. (E) Remove the catheter and unclamp. Arterial blood flow through IVC stenosis can be observed. Please click here to view a larger version of this figure.
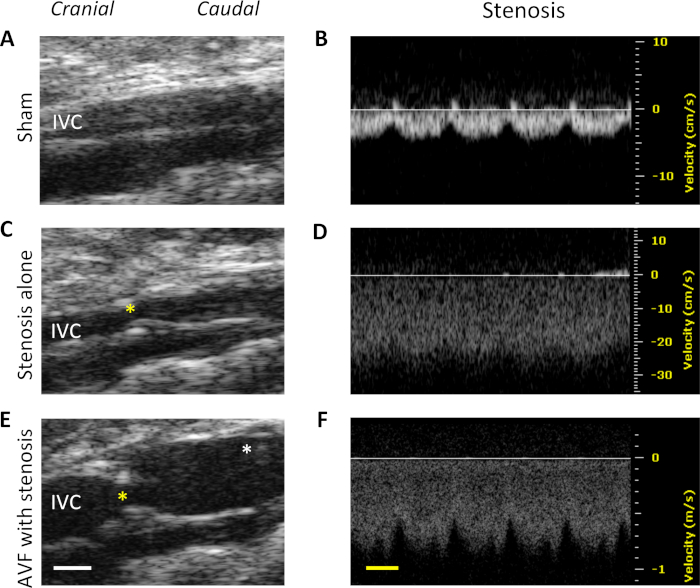
Figure 2. Ultrasound findings on day 7 after the surgical procedure. Top: representative images of mice with a sham procedure. (A) B-mode image shows IVC in the longitudinal view. The left side is the cranial side. (B) Waveform of the infrarenal IVC. Middle: representative images of mice with a stenosis alone. (C) B-mode image shows IVC including the stenosis (yellow asterisk) in the longitudinal view. The left side is the cranial side. (D) Waveform in the area of the stenosis. Bottom: Representative images of mice having AVF with stenosis. (E) B-mode image shows IVC including fistula (white asterisk) and stenosis. The left side is the cranial side. (F) Waveform in the area of the stenosis. White scale bar represents 1 mm. Yellow scale bar represents 100 ms. Please click here to view a larger version of this figure.
| Stenosis | Yes | Yes | P value |
| AVF | No | Yes | |
| Time-averaged maximum velocity (mm/s) | 180 | 878 | 0.0023 |
| Stenosis diameter (mm) | 0.62 ± 0.01 | 0.63 ± 0.01 | 0.3558 |
| % stenosis (upsteam) | 43% | 66% | 0.0159 |
| % stenosis (downsteam) | 42% | 56% | 0.0006 |
Table 1. Ultrasound measurement at the IVC stenosis area of each group. Ultrasound derived measurements at the IVC stenosis area of mice having stenosis alone and mice having AVF with stenosis on day 7 after surgery. %stenosis (upstream) = (1 – [diameter at stenosis / diameter at upstream reference segment]) x 100%. %stenosis (downstream) = (1 – [diameter at stenosis / diameter at downstream reference segment]) x 100%. %dilation = (diameter on postoperative day 7 / preoperative diameter at the same segment) x 100%. P values are based on Student’s t-tests, n = 4-6.
