The identification of a route to sterilize the skin before setting up the wound infection model was challenging. The challenge lay in sterilizing the skin without damaging the different skin layers, which may then go on to have unintended consequences in the outcome of infection. To identify an appropriate sterilization regime, different treatments were tried for varying lengths of time, as outlined in Table 1. Contamination was recorded as the development of turbidity after 48 h in the MK medium used to maintain the skin samples. Tissue integrity was monitored by histology followed by staining with hematoxylin and eosin (H&E) immediately after treatment (Figure 1). A 30 min treatment with chlorine dioxide proved the most effective at reproducibly sterilizing the skin tissue whilst preserving tissue integrity.
In the experimental setup, the wounded sterile tissue is placed in the apical chamber of a 24-well insert at the air-liquid interface (Figure 2A). Two different wounding techniques were attempted-a flap removal technique, in which the tissue is wounded by a punch biopsy tool and the top layer of the wounded tissue is removed using a combination of a 15-blade scalpel and sterile toothed allis tissue forceps, and a scratch technique, in which the tissue is wounded by a punch biopsy tool alone. Although the scratch model harbored a higher average number of CFUs after 24 h, the results were variable. The flap removal technique produced more consistent results (Figure 2C). After 48 h, approximately 100 times more bacterial CFUs were recovered from the wounded tissue compared to the inoculum (Figure 2D). This was deemed to indicate a successful infection. A white film in the wound bed was evident on the tissue 48 h after infection (Figure 2B). Gram-stained histology sections of infected tissue indicated the presence of S. aureus cells in the wound bed (Figure 2E,F). Gram-stained histology sections of uninfected tissue are provided as a comparator (Figure 2G,H).
From one lamb's head, a 100 cm2 section (10 cm x 10 cm) can be realistically accessed. Given each patch of skin is punched out of the forehead using a circular 8 mm diameter punch biopsy, approximately 100 skin patches can be obtained from one lamb's forehead per week. Procuring further lambs' heads proportionately increases the number of skin samples that can be obtained per week. Hence, it is claimed that the procedure is relatively high throughput. For this study, 24 skin samples were obtained routinely per week. Skin from various lambs' heads was processed as biological replicates to account for the potential donor to donor variability. During the preparation of the skin patches (steps 3.1-3.8), the major time consumption is the 30 min incubation of the skin samples in the chlorine dioxide solution and the 2 x 35 min wait for the hair removal cream treatment. The use of punch biopsy to generate the 24 skin patches takes about 15 min. It is this time that would scale linearly if the number of skin patches were increased.
| Disinfectant | 10 Min | 30 Min | 60 Min |
| 1% high-level medical surface disinfectant | F | P | P |
| 1% multi-purpose disinfectant | F | F | P |
| 3% povidone | F | F | F |
| 5% povidone | F | P | P |
| 10% povidone | F | P | P |
| 70% ethanol | F | P | P |
| UV | F | F | F |
| 0.55% hypochlorite | F | P | P |
| 200 ppm chlorine dioxide | F | P | P |
Table 1: Sterilization of fresh lamb skin. Each skin sample was left in the disinfectant for the specified time. F denotes failure to sterilize the tissue, with bacterial contamination present in the media. P denotes passing, with no bacterial contamination present in the media.
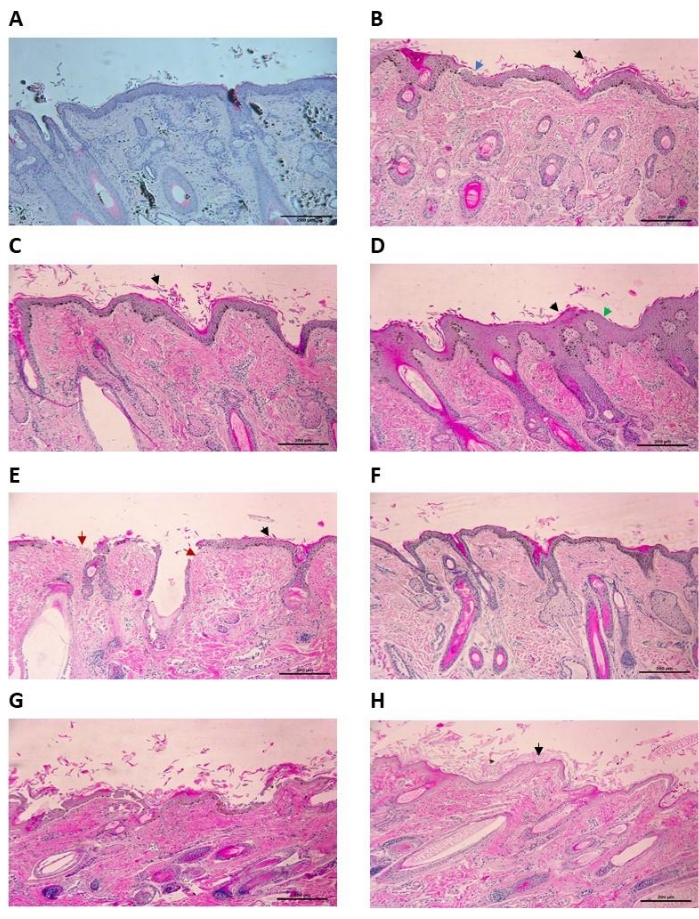
Figure 1: Histology of uninfected ex vivo ovine skin treated with disinfectants (H&E stain) at 100x magnification. (A) Control skin sample with 30 min treatment in PBS. Some epidermal shedding can be seen, but the epidermis is not disrupted. (B) Ovine skin treated with 1% high-level medical surface disinfectant for 30 min. Epidermal shedding (black arrow) along with some disruption to the stratum granulosum (blue arrow). (C) Ovine skin treated with 5% povidone for 30 min. Moderate damage to the tissue can be seen here, with epidermal shedding of the stratum corneum (black arrow). There is minimal disruption to the underlying epidermal layers. (D) Ovine skin treated with 10% povidone for 30 min. The top layers of the epidermis have been damaged, with evidence of shedding (black arrow) and thinning (green arrow). (E) Ovine skin treated with 2% multi-purpose disinfectant for 30 min. Severe damage to the sample can be observed, with significant epidermal shedding (black arrow) and complete eradication of the stratum corneum (red arrow). (F) Ovine skin treated in 200 ppm chlorine dioxide for 30 min. Some epidermal shedding can be seen, but the epidermis is intact. (G) Ovine skin treated with 0.6% hypochlorite for 30 min. Severe damage to the epidermis is present, with a high level of epidermal shedding (black arrow) and eradication of the epidermis in places (red arrow). (H) Ovine skin treated with 70% ethanol for 30 min. Damage to the epidermis can be seen, with significant epidermal shedding (black arrow). Scale bar is 200 µm. Please click here to view a larger version of this figure.
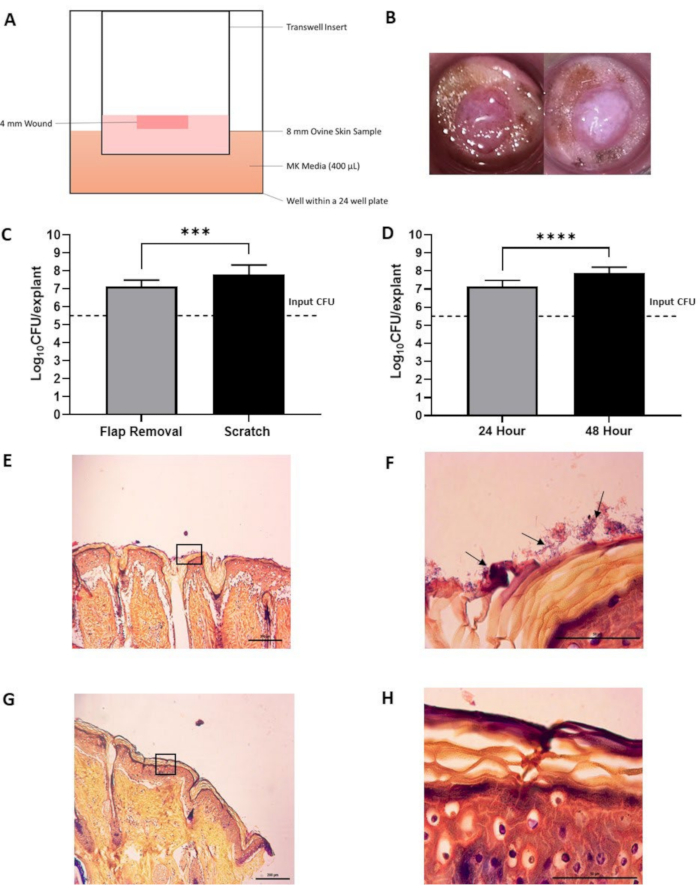
Figure 2: Ex vivo ovine skin infected with S. aureus. (A) Schematic of the experimental setup. (B) Pictures of ex vivo ovine skin prior to infection (left image) and post 48 h infection (right image). Note the white film present following 48 h incubation in infected tissue, which is absent in uninfected tissue. (C) Testing the effect of different wounding methods on the final colony forming unit (CFU) counts after homogenization. Flap removal (n = 6) and scratch (n = 9) infected with S. aureus for 24 h. Error bars indicate standard deviation. *** indicates a p-value < 0.0001. (D) Testing the effect of incubation times on CFU counts following homogenization. 24 h incubation (n = 6) and 48 h incubation (n = 12). Error bars indicate standard deviation. **** indicates a p-value < 0.0001. (E,F) Representative images of histopathological analysis of infected ovine skin post 48 h infection with a modified Gram stain (E) at 100x magnification (scale bar of 200 µm). The box indicates the area magnified in (F) at 1,000x magnification (scale bar of 50 µm). Black arrows indicate bacteria. (G,H) Representative images of histopathological analysis of uninfected ovine skin following a 48 h period (control) with a modified gGram stain (G) at 100x magnification (scale bar of 200 µm). The box indicates the area magnified in (H) at 1,000x magnification (scale bar of 50 µm). Statistical analysis was carried out as a one-way ANOVA. Please click here to view a larger version of this figure.
